
Dopo tre anni di passione e preparazione, dopo mesi di distillazione, il passaggio dal progetto OfficinaLessinia al marchio Gadoi è fatto. Siamo finalmente approdati alla fase finale, quella della commercializzazione dei prodotti da filiera locale, ossia oli essenziali ed acque aromatiche da piante biologiche e/o da raccolta spontanea sostenibile. Al momento offriamo un listino che si compone di 12 oli essenziali ed acque aromatiche provenienti dalle montagne della Lessinia (Verona) e 4 oli essenziali della Sardegna. Con il 2017 contiamo di aggiungere alcuni oli essenziali selezionati provenienti dalle filiere controllate del Nepal che abbiamo visitato nel 2016 e che visiteremo nell’anno prossimo. Sempre nel 2017 offriremo miscele funzionali di oli essenziali per applicazioni topiche e per assunzione orale in forma di microincapsulati gastroprotetti. Siamo orgogliosi di offrire solo piante locali, sia derivate dal pool genetico del territorio, sia da una selezione di cultivar o chemiotipi che abbiamo selezionato per la loro adattabilità. Il lancio ufficiale del sito di e-commerce e del database sugli oli essenziali (www.gadoi.it) avverrà a fine gennaio, e da quel momento sarà possibile accedere liberamente ai dati gas-cromatografici dei singoli lotti di oli essenziali ed acque aromatiche, oltre che ai riferimenti in letteratura sulle caratteristiche dei prodotti. Per chi fosse interessato al listino prezzi prima della pubblicazione del sito, è possibile riceverlo contattandoci alla mail info@gadoi.it Ringraziandovi per l’interesse mostrato per il nostro progetto, vi auguro Buone Feste.
Oli essenziali ed aromaterapia: i nuovi corsi 2016-2017
Il blog viene nuovamente risvegliato, dopo mesi di letargo, per una nuova promozione. Come ho spiegato nell’ultimo post del 2015, questo intervallo di inattività è coinciso con la nuova attività nel progetto di sviluppo della Lessinia attraverso la coltivazione e la distillazione di piante aromatiche. Il progetto è arrivato ad una nuova fase, che coincide da un lato con la nascita di una srl di produzione di oli essenziali ed acque aromatiche a filiera corta e controllata, a nome Gadoi, e dall’altra dalla programmazione di un nuovo corso di studi sugli oli essenziali. A differenza delle proposte degli altri anni, questa volta abbiamo deciso di concentrarci sulla parte degli oli essenziali e delle loro applicazioni pratiche, indirizzandoci quindi in maniera più specifica verso professionisti del settore che offrono o consigliano oli essenziali, quali erboristi, farmacisti e medici, o che li utilizzano direttamente, quali massaggiatori, fisioterapisti, personale di sauna, ecc.
Abbiamo anche deciso di scomporre il programma completo, che avrebbe avuto una durata di circa 10-12 fine-settimana, in una serie di seminari autonomi che possono essere fruiti indipendentemente dagli altri, ma che insieme formano un corso di studi organico e completo.
Subito qui sotto potete leggere o scaricare il depliant informativo generale su tutti i corsi


mentre qui sotto potete scaricare calendario e prezzi
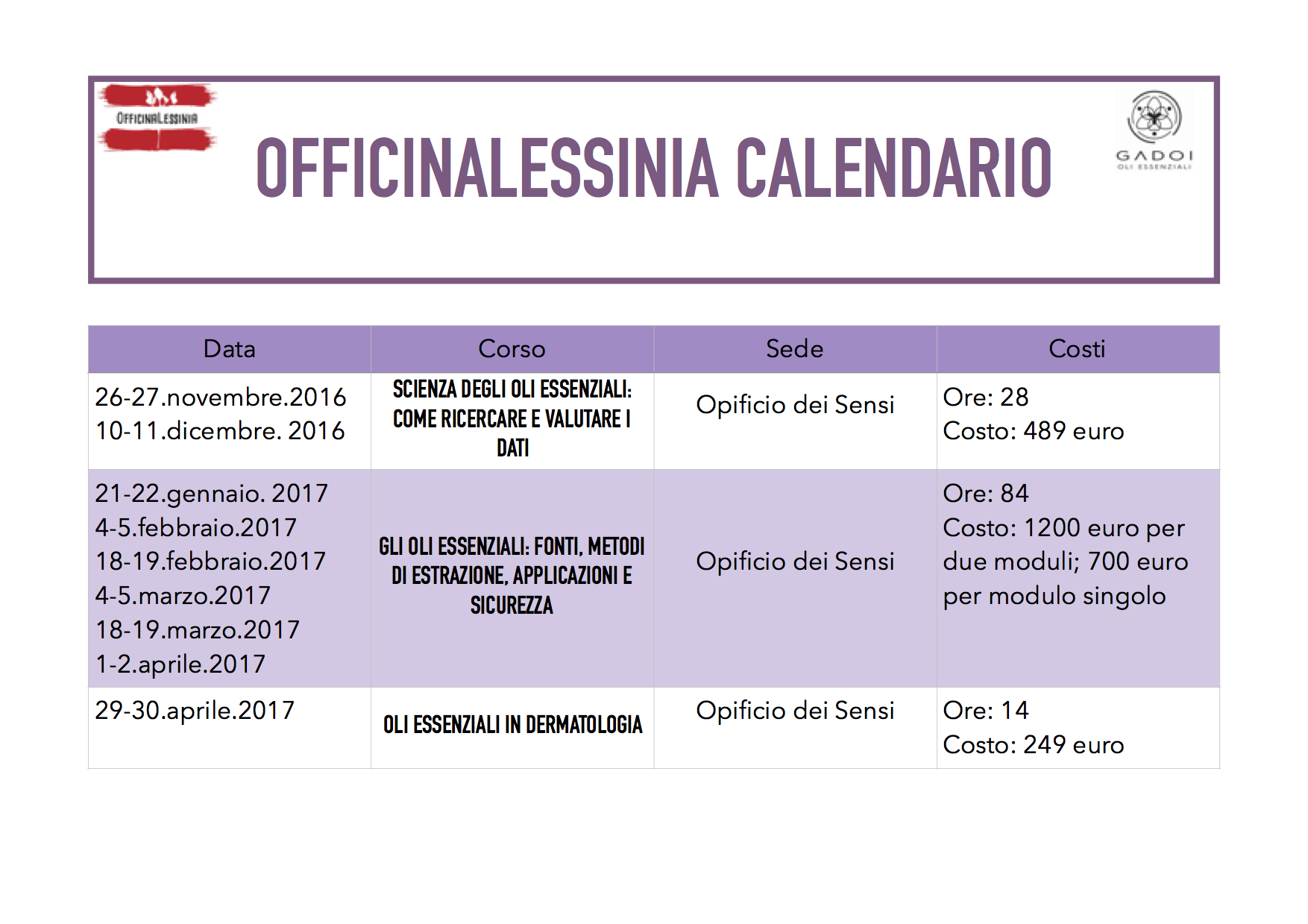

Il primo seminario in programma: “Scienza degli oli essenziali: come ricercare e valutare i dati” è propedeutico per tutti gli altri moduli, e si concentra su come fare, interpretare ed usare la ricerca in campo biomedico, storico ed etnobotanico, ed è stato pensando con gli erboristi ed altri professionisti in mente, anche se è aperto a chiunque sia interessata/o alla valutazione scientifica dei dati sulle piante medicinali. La prima parte del corso sarà incentrata sulla ricerca ed i suoi metodi, mentre la seconda parte si concentrerà sugli strumenti a nostra disposizione per fare ricerca o interpretare la ricerca fatta da altri, con particolare attenzione al mondo delle piante aromatiche e degli oli essenziali. Il seminario prevede varie ore di lezione frontale, ma alle studentesse e agli studenti sarà richiesto un certo lavoro a casa, letture ed applicazioni dei concetti studiati in classe.
La durata del corso sarà di 2 fine-settimana per un totale di 28 ore di lezione frontale, e il costo sarà di 489 euro IVA inclusa. Si terrà presso la Cooperativa Opificio dei Sensi di Verona e sarà così strutturato:
Presentazione
Introduzione alla interpretazione della letteratura scientifica come strumento di autoformazione permanente e di valutazione delle informazioni offerteci dal mercato.
Esso si compone di quattro sezioni principali che affrontano i temi più importanti per lo studio delle piante medicinali e degli oli essenziali:
- le origini delle trappole mentali, il ruolo della disciplina e del pensiero critico nella ricerca;
- la logica della medicina;
- lo studio dei dati folclorici e storici per la valutazione della tradizione erboristica, e l’analisi della ricerca biomedica, dell’epidemiologia e dei principali strumenti per la valutazione di efficacia e sicurezza dei rimedi
- una disamina delle fonti e degli strumenti più rilevanti in internet.
Programma
Le basi: il ruolo della scienza nella ricerca
- “Trappole mentali”
- Credere, dubitare e sospendere il giudizio
- Dalla superstizione alla filosofia naturale, dai fiumi di Babilonia al Medioevo europeo, alla Scienza Moderna.
- La scienza non è una vacca sacra e neppure un “discorso” tra tanti.
- Cosa è il metodo scientifico? Ovvero, ne esiste uno?
Le basi: la logica della medicina
- Cause.
- Malattia e normalità.
- Prove.
- Bias.
- Confounding.
Ricerca biomedica
- Una introduzione all’epistemologia e alla biostatistica
- Definire i tipi di studio
- Studi in vitro ed in vivo.
- Studi clinici.
- Metastudi.
- Limiti e punti di forza dei vari studi.
- Descrivere i dati
- Una comprensione intuitiva dell’analisi statistica
- Il primo passo: testare le ipotesi e livelli di confidenza
- L’interpretazione e la valutazione dell’accuratezza dei dati:
- Come leggere gli studi e come attribuire valori di evidenza e di rilevanza agli
- studi.
- Come costruire una gerarchia delle evidenze.
- Cenni ai problemi più generali della ricerca.
- Discussione delle piante con maggior sostegno scientifico
Ricerca in etnobotanica ed etnofarmacologia
- Introduzione ad etnobotanica ed etnofarmacologia: l’importanza delle piante per l’uomo, definizioni, storia, metodi, fonti
- L’etnobotanica contemporanea: filoni di ricerca, problemi, relazione con la fitoterapia
- Metodi in etnobotanica applicata: gli strumenti per fare da sole ricerca sul campo delle tradizioni locali
- Discussione delle piante che hanno fatto la storia dell’etnofarmacologia
Il reperimento delle fonti nell’era di internet
- Internet ed il paradosso dell’eccesso di informazione
- Strumenti per selezionare i siti sicuri
- Elenco ragionato di fonti sicure divise per argomento
Lo stato dell’arte nella ricerca sugli oli essenziali
- Una panoramica sulla ricerca preclinica e clinica in aromaterapia.
Un nuovo sforzo
Il periodo di silenzio di questo blog è coinciso, come spesso accade, con un periodo di grande attività su altri fronti. Ecco quindi che il primo post dopo tanto tempo è un post di annunci.
Dopo lungo rimuginare, insieme a dei compagni di avventura abbiamo deciso di intraprendere un percorso prima divulgativo e poi si spera imprenditoriale che si centra sulle piante aromatiche e sui loro derivati, principalmente oli essenziali e acque aromatiche.
Il progetto è nato un paio di anni fa da una chiacchierata tra amici sulle spiagge Salentine. Si parlava di terreni e territori abbandonati, degradati, e di persone costrette ad abbandonarli perché non più in gradi di essere produttivi al di là di una agricoltura di sussistenza oppure della coltivazione dell’ulivo e della vite. Nacque li il primo nucleo del progetto: come pensare a coltivazioni e filiere diverse, innovative, in grado di assicurare un margine economico sufficiente a convincere le persone a rimanere sul territorio?
Successivamente abbiamo spostato il nostro obbiettivo dal Basso Salento alle montagne della Lessinia nel Veronese, per ovvi motivi: siamo di Verona. Ma il concetto è lo stesso, ed è facilmente traducibile per i territori montani, che soffrono di problemi molto simili ed a volte accentuati rispetto ad altre aree geografiche.
Nel territorio della Lessinia le attività agricole si sono andate riducendo da molto tempo, per la diaspora dei giovani e per le difficoltà economiche e la concorrenza di altri attori sul mercato, tanto che anche la coltivazione e la prima trasformazione delle piante officinali difficilmente permettono un reddito significativo.
Vista la mia formazione non sorprende che io abbia pensato alle piante officinali, che teoricamente hanno un prezzo alla vendita maggiore di prodotti orticoli, e non hanno bisogno di grandi cure agricole, anzi. Ma precedenti esperienze mi avevano insegnato che il discorso non era così semplice. Per dirne una, produrre solo pianta essiccata rende pochissimo, dato che molte aziende italiane acquistano all’estero anche piante nostrane per i prezzi decisamente inferiori. L’unico modo sembrava quello di bypassare le aziende di trasformazione e di pensare ad una filiera conclusa il più possibile nel territorio, il più possibile corta, in modo da tagliare i costi degli intermediari e soprattutto di tenere a se la trasformazione, che è il processo che aumenta di più il valore aggiunto della merce. Si trattava quindi di pensare ad una azienda agricola o consorzio agricolo ad elevata concentrazione di competenze, e allo stesso tempo di identificare un processo produttivo non troppo costoso, complesso e burocraticamente oneroso.
Abbiamo quindi pensato alla distillazione per i sopracitati motivi. La distillazione ha molti vantaggi su altri tipi di trasformazione:
- è fino ad ora permessa all’agricoltore come parte delle sue normali attività,
- non abbisogna, almeno agli inizi, di laboratori dedicati,
- non abbisogna, almeno agli inizi, di investimenti tecnologici molto elevati o di autorizzazioni particolari
- l’agricoltore può scegliere di vendere l’OE al cliente nel suo spaccio o al mercato (e non ha bisogno di alcun laboratorio) mentre per venderlo a terzi serve un piccolo laboratorio
- di contro permette di ottenere un prodotto che si conserva a lungo, che occupa poco spazio e può quindi essere facilmente spedito verso altre zone, e che ha un elevato valore aggiunto.
Ecco perché abbiamo pensato che la coltivazione di specie aromatiche espressamente mirate ad un mercato degli OE sia una buona idea, che naturalmente andrebbe accompagnata da uno sforzo a più ampio raggio, con offerta di altri prodotti (altri tipi di estratti, prodotti contenenti OE, acque aromatiche, pianta in taglio tisana, mazzetti) e servizi (formazione, informazione sulle piante e sulla storia del territorio, visite guidate, ecc.)
A nostro parere portare in questi territori una filiera più completa permetterebbe di ottenere un margine di guadagno maggiore per il coltivatore rispetto alla vendita del foraggio.
Inoltre si favorirebbe un ritorno dei giovani nel territorio ed un legame con le attività di ricezione turistica, specie quelle più ‘green’ che tirano oggi il mercato, anch’esse in grande difficoltà[1]. Contribuirebbe inoltre a ridurre il fenomeno dell’abbandono delle superfici agricole, al recupero di terreni abbandonati (seminativi, pascoli, boschi, ecc..), alla diminuzione del rischio di antropizzazione, allo sviluppo di un’attività culturale, formativa ed educazionale[2] volta al recupero delle tradizioni dell’utilizzo delle erbe medicamentose ed essenzifere della Lessinia[3]. Un patrimonio culturale di conoscenze sulla medicina naturale, sull’uso delle piante officinali (PO) utilizzate in Lessinia si va perdendo.
Abbiamo quindi formato una associazione, denominata OfficinaLessinia (qui il sito e la pagina FB), che intende organizzare corsi ad hoc per gli operatori dell’agricoltura, atti a fornire loro il necessario background scientifico, tecnico e tecnologico, oltre che di strategie commerciali, per intraprendere l’attività di coltivazione e trasformazione (distillazione e altro) di PO in maniera da massimizzare la qualità del prodotto e il guadagno, puntando su specie autoctone.
Ecco qui i link ai primi post, qui e qui.
![]()
Soprattutti però ci proponiamo di promuovere una nuova attività economica locale, basata su almeno tre caratteristiche peculiari cioè punti di forza della Lessinia:
1. Caratteristiche botaniche peculiari per la produzione di alcune specie officinali caratteristiche e storiche della Lessinia (es. giaggiolo veronese, o Iris xgermanica L.), ad elevato valore aggiunto perché molto ricercato dalle più grandi e famose case profumiere francesi, sulla quale impostare l’attività di marketing-comunicazione dell’associazione. Si punta a far diventare la Lessinia la capitale italiana del giaggiolo, gareggiando con la zona del Chianti senese: lì l’abbinata vino-profumo sta funzionando e non si vede come anche a Verona, terra di vini, non si possa creare una sinergia simile, pur con le dovute proporzioni. In più, rispetto alla produzione di OE della Toscana, la Lessinia potrebbe vantare prodotti essenziferi di alta quota (in Lessinia si arriva fino a quote alpine, non così nel Chianti o nel senese toscano) ad alto contenuto di sostanze pregiate (come lavanda d’alta quota, mugo, abete, Achillea clavennae-nativa della Lessinia), da commerciare in abbinamento con gli altri prodotti.

Iris germanica L.
2. Caratteristiche del territorio:
- ben circoscritto (Val d’Adige a Ovest – Val d’Illasi / d’alpone a Est)
- ben riconoscibile per le sue caratteristiche inconfondibili del paesaggio (colline erbose dolci solcate da vaj boscosi profondi e, più in alto, le caratteristiche formazioni di lastre di pietra di Prun)
- esente dall’inquinamento di aria e terra della pianura (un fattore su cui puntare nella comunicazione di prodotti per il benessere e la salute)
- parco regionale della Lessinia
- vicinanza alla quarta città turistica d’Italia e importante snodo commerciale e viario.
3. Caratteristiche pedoclimatiche ideali per la crescita di piante officinali ad alto contenuto di sostanze pregiate:
- differenziale termico estate – inverno
- terreni in altitudine 700-1600 m slm
- pascoli ad elevata insolazione e moderata-forte ventilazione
- clima montano ma di tipo temperato (ricalcante l’Appennino)
Non si intende scoprire nulla di nuovo, ma rispolverare vecchie ricette ancora valide: le piante aromatiche sono infatti state individuate fin dagli anni ’70 da eminenti esperti ed economisti locali quale il possibile motore trainante di un’economia della montagna veronese[4].
Riguardo alle piante a cui miriamo, nel futuro, come detto, vorremmo occuparci di Iris, vista l’antica tradizione di coltivazione e trasformazione del rizoma di giaggiolo in area est-Lessinia (‘gadoi’), ma conoscendo le difficoltà della filiera (5-6 anni), pensiamo di doverci arrivare con calma. Abbiamo iniziato con la Lavanda vera ed il Lavandino, mentre stiamo pianificando la raccolta e la coltivazione di Achillea millefolium, Carum carvi, Artemisia vulgaris, Pinus mugo, Abies spp., Daucus carota, Mentha spp. e Melissa officinalis.
Inoltre abbiamo già costituito una rete di collaborazioni con il Salento (dove abbiamo appena tenuto varie giornate di corsi-incontri-distillazione sul progetto con circa 130 persone intervenute), in Sicilia e Sardegna per la commercializzazione di OE che qui al Nord non ha senso produrre (elicriso, lentisco, mirto, timo, origano, agrumi, ecc..), e quindi in futuro da affiancare al progetto in Lessinia. Andremo perciò a commerciare un marchio unico con prodotti da piante di diverse provenienza, ma controllate e disciplinate dallo stesso protocollo.
———————
Note
[1] Si punta ad incrementare l’afflusso di turisti e persone interessate alla cultura della montagna o che trovano nei prodotti della Lessinia quella componente di artigianalità e di cura per i dettagli difficili da reperire altrove. Le aziende che fanno accoglienza potranno aggiungere una nuova linea per il benessere e la salute prodotta interamente da loro. Garantiti dal marchio della nostra impresa, votata al nobile fine di valorizzare, tutelare e promuovere ambiente e società della montagna veronese.
[2] corsi di formazione su coltivazione, distillazione, utilizzi, storia della flora, ecologia, raccolta sostenibile, recupero di specie autoctone e simili di Piante Officinali (PO) e Olii Essenziali (OE), diretti a agricoltori, erboristi, farmacisti, medici, naturopati, operatori della filiera delle PO, cittadini interessati ad acquisire conoscenze su utilizzo delle PO.
[3] Medicina popolare: studio etnobotanico nel parco della Lessinia, Relatore Stefano Bona, Facoltà di agraria e farmacia, Padova, 2004
[4] Vita Veronese, le piante officinali della Lessinia, 1978; Quaderno dei Cimbri, ed. Tzimbar,1998.
Qualche corso qua e là…
Aggiorno gli interessati sui corsi che terrò nel prossimo futuro:
- Venerdì 28 Marzo sarò in quel di Arezzo presso il 7° Forum della FIPPO a parlare di oli essenziali e delle loro applicazioni, qui trovate il programma con tutti gli altri relatori.
- Lunedì 3 Marzo inizia invece a Verona il corso (in quattro seminari) sulla trasformazione delle piante officinali, un corso teorico-pratico pensato specialmente per gli erboristi ma aperto a tutti gli interessati. I seguenti seminari saranno il 17 e 31 Marzo ed il 14 Aprile. Qui sotto la scheda di iscrizione della SISTE.


- Il 16 Marzo sarò a Bologna allo Smell Atelier con due seminari, uno alla mattina sugli utilizzi degli olii essenziali e uno al pomeriggio sul tema delle resine e degli incensi nella storia. Qui il link alla presentazione. Il 6 Aprile sarò di nuovo allo Smell Atelier a parlare prima di neurogastronomia e poi di spezie.
Gummi Myrrha
Continua con questa seconda parte il pezzo sulla mirra, che inizia qui.
Mirra oggi: definizione e descrizione
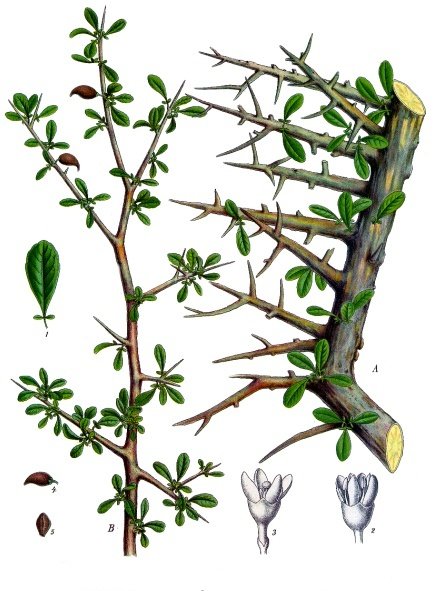
Ci sono 190 specie di Commiphora (famiglia delle Burseraceae) distribuite in Africa, India, Penisola Arabica usate tradizionalmente come incenso e medicina. La mirra (Gummi Myrrha) è la gommo-oleoresina essiccata all’aria ottenuta dai fusti e dai rami di Commiphora myrrha (Nees) Engl. (sinonimi Balsamea myrrha (T.Nees) Oken;B. myrrha Baill.; B. playfairii Engl.; Balsamodendrum myrrha T.Nees; Commiphora coriacea Engl.; C. cuspidata Chiov.; C. molmol (Engl.) Engl. ex Tschirch[82].
Questa specie è un albero indigeno dell’Africa Nordest (Gibuti; Etiopia; Somalia e Kenya), in particolare di Somalia ed Etiopia (e in misura minore Sudan)(CHP) e dell’Arabia meridionale (Oman; Yemen). La droga, a volte di qualità inferiore, si ricava però anche da altre specie: Commiphora habessinica (O.Berg) Engl.; (sinonimoC. abyssinica); Commiphora schimperi (O.Bergman) Engl.; altre inferiori C. foliacea Sprague, Commiphora playfairii (Hook.f.) Engl C serrulata Engl.. Commiphora africana (A.Rich.) Endl in Etiopia e Sudan.

La pianta cresce fino a 3 metri di altezza o più anche se si conoscono forme nane, e porta foglie dentate verdi. Fessure e spaccature si formano naturalmente nella corteccia dalle quali la resina essuda naturalmente dai dotti circolari del parenchima, ma la resa aumenta con le incisioni.
Nomi popolari: Myrrh, Myrrha, Myrrhe, African Myrrh, herabol Myrrh, Somali Myrrh, Smyrna, Mur, Murry, Bola o Bol, Vola, Murr, Mirra. olio di Mirra, Stacte.
Raccolta: la resina di mirra, come quella dell’incenso, viene raccolta incidendo la corteccia e lasciando che la resina fuoriesca, si raccolga e si indurisca, in due o tre settimane. A questo punto può essere staccata e raccolta. Questo metodo, ancora in uso oggi, è stato descritto per la prima volta da Teofrasto e più tardi da Erodoto.
Le masse raccolte sono rosso-marroni, vengono ammassate in sacche fatte di pelle di capra e mandate quasi esclusivamente ad Aden. La qualità di Mirra più ricercata è la “ogo”, proveniente dalle aree interne lontane dalla costa somala e da Guban[83]. Tempo addietro le masse resinose (gocce o lacrime di mirra) venivano esportate da Aden in paesi stranieri dove venivano lavorate per produrre resinoidi ed olii.
La Somalia è il più grande esportatore al mondo di Mirra, Opopanax (Commiphora kataf (Forssk.) Engl., [= C. erythraea (Ehrenb.) Engl.], Olibanum (Boswellia sacraFlueck. [=B. carteri Birdw.]) e Maidi (B. frereana Birdw.). Le specie di Commiphoraso trovano nelle località interne secche dal nord all’estremo sud, ma buona parte del materiale esportato dalla Somalia viene in realtà raccolto in Etiopia. Alla fine degli anni 80 il volume di resine di Commiphora esportato ammontava a 1000 tonnellate[84]
La gommo-resina
La sesta edizione della Farmacopea Italiana[85] distingue tra mirra eletta emirra in sorte. La prima “si presenta in grani (lagrime) od in pezzi irregolari di varia grossezza, di colore rossastro o rosso-bruno, screpolati, un po’ efflorescenti, alquanto traslucidi, fragili, di frattura lievemente granellare e lucida, con alcune vene o piccole macchie biancastre o giallicce, talore semilunari. Sapore amarognolo, odore aromatico.
La mirra in sorte è formata di masse conglomerate, brune, opache, miste a frammenti di corteccia ed a varie impurità.”
Le Monografie dell’OMS sulle piante medicinali[86] così la descrivono: “Gummi Myrrha consiste nelle oleo-gommo-resine essiccate all’aria essudate da fusti e rami della Commiphora molmol Engler (Burseraceae) ed altre specie di Commiphora correlate, incluse C. abyssinica Engl., C. erythraea e C. schimperi Engl., ma escludendo C. mukul.” La gommo-resina si presenta come: “gocce o grumi di gocce irregolari o arrotondate di varie dimensioni, di colore da giallo-marroncino a rosso-marrone fino a quasi nero. La superficie è quasi completamente coperta di polvere grigiastra o giallognola; la superficie interna è giallastra o rosso-marrone, che a volte presenta macchie o linee bianche; la frattura è cerosa, granulare, concoidale (a superficie curva) e dà frammenti sottili e traslucenti”.
L’odore è caratteristico, caldo-balsamico, dolce e con toni speziati, aromatico e pungente quando la resina è fresca; il sapore è aromatico, amaro, aspro[87].
La gommo-resina si scioglie parzialmente in acqua, alcol ed etere.



La resina viene usata come nota di base speziata con carattere orientale, come base legnosa, di foresta, di aghi di pino. Si associa bene a geranio, muschio, patchouli, spezie e basi floreali pesanti[88].
Prodotti derivati[89]
La distillazione in corrente di vapore della gommoresina produce il classico olio di mirra, con rese da 1,5% a 15%, ma grazie a recenti tecnologie (come ad esempio distillazione controcorrente “short-path” o “gas-swept” si producono nuove qualità con rese molto elevate.
Olio di Mirra: liquido vischioso giallo con odore caratteristico della gommoresina, cioè resinoso e dolce balsamico, ma con anche un aspetto amaro/astringente. Odore molto persistente. Nota finale debole, secca, legnosa tipo vetivert.
Resinoide di Mirra: ottenuto per estrazione della gommoresina con solventi volatili (nel passato toluene ed esano); è un solido rosso-marrone con odore dolce, balsamico, di zucchero integrale, e uno sfondo oleoso, legnoso e terpenico. La nota finale è dolce, in qualche modo caramellosa, terpenica e di muffa.
Tintura di Mirra: preparata per macerazione della mirra in polvere con alcol etilico a 80°. Appare un liquido di colore rossastro non molto intenso. Odore e sapore di mirra, reazione acida al tornasole; diluita con acqua si intorbida[90].
Composizione chimica
Come per le specie appartenenti al genere Boswellia, anche nelle specie diCommiphora l’essudato contiene polisaccaridi ed è quindi classificato come gommoresina. Una volta indurita è scura e amara al contrario della gommoresina diBoswellia che è pallida e dolce.
La gommoresina è frazionabile in tre parti, due liposolubili ed una idrosolubile:
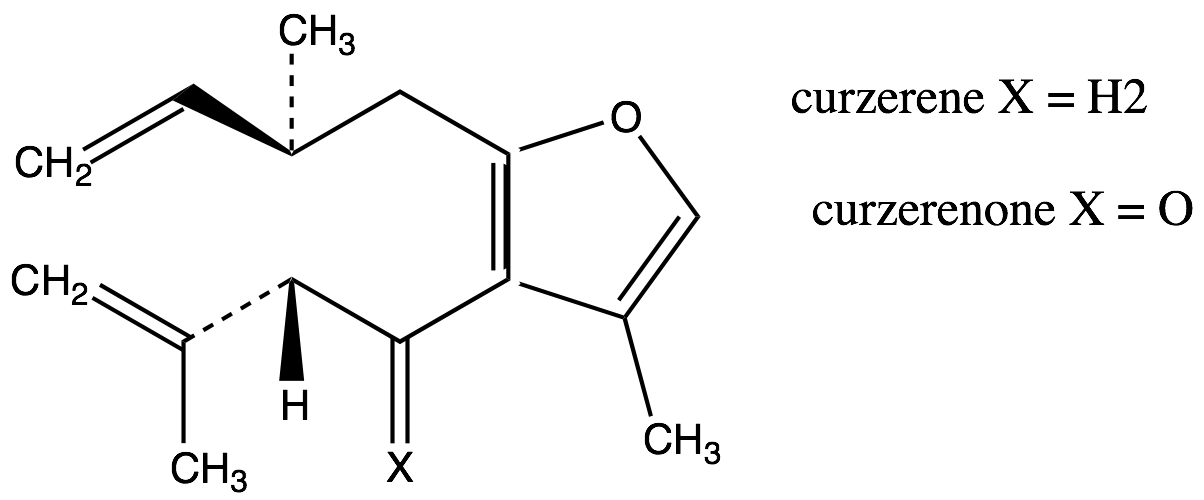
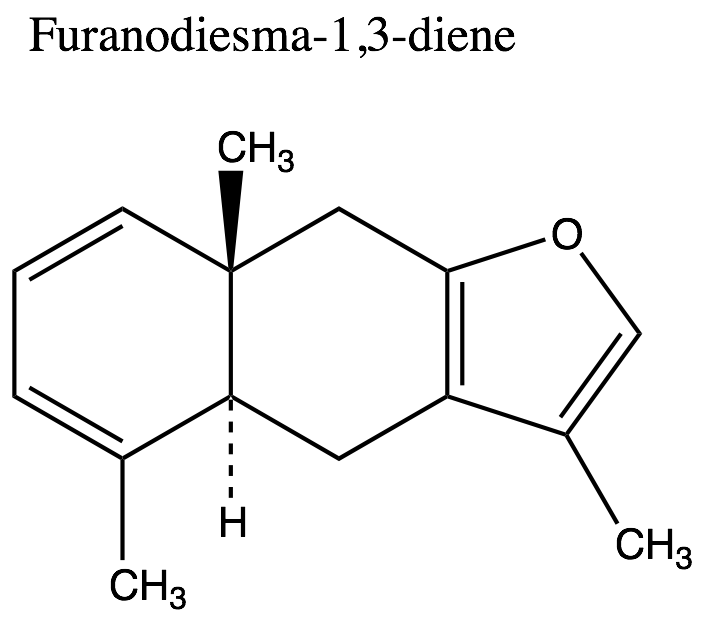
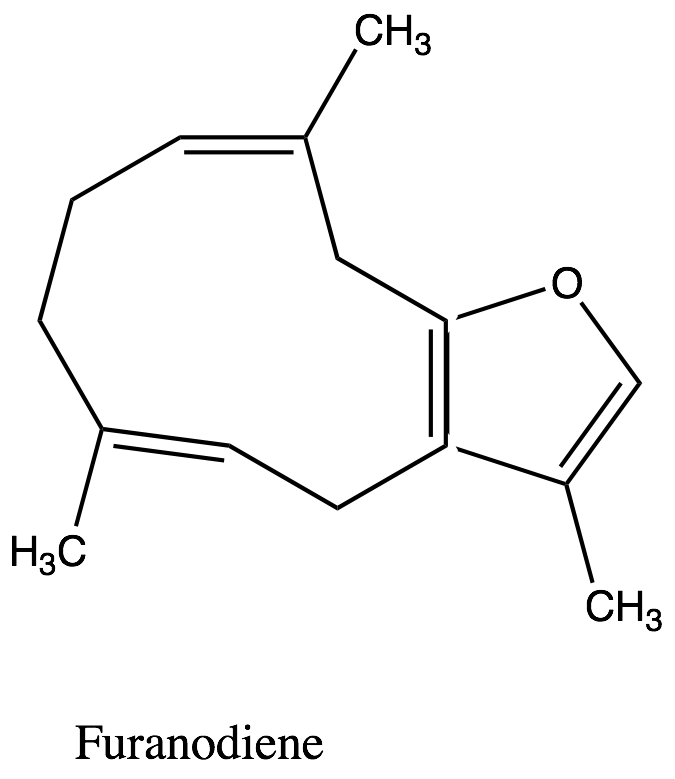
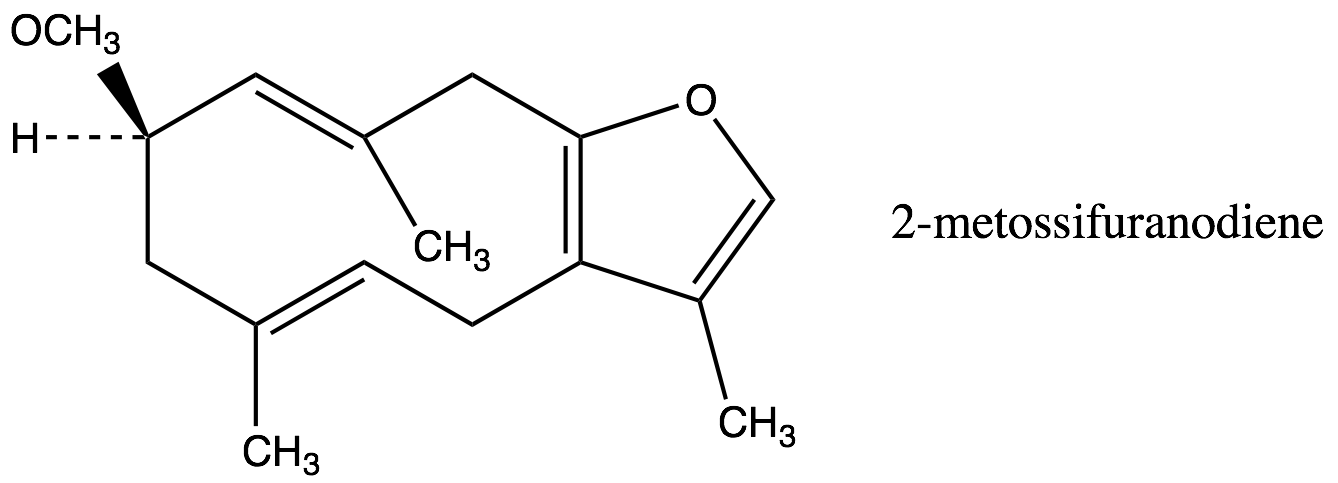
1. Frazione volatile liposolubile, o olio essenziale (1,5-17% – forbice più comune 3-8%): caratterizata sia dai monoterpeni sia dai sesquiterpeni. Tra i monoteropeni troviamo α-, β- e γ−bisabolene, α-pinene, dipentene e limonene, mentre tra i sesquiterpeni troviamo heerabolene, cadinene, curzerene (11.9%), curzerenone(11.7%), diidripirocurzerenone (1,1%), elemolo, beta-elemene, T-cadinolo, commiferinae vari furanosesquiterpenoidi tra i quali il furanoeudesma-1,3-diene (12.5-34.9%), il furanodien-6-one (0.4% ), il furanoeudesma-1,4-diene-6-one, l’isofuranogermacrene, il 1,10(15)-furanodien-6-one, il 2-metossi furanodiene, illindestrene (3.5-12.9%), ecc. Sono presenti anche composti fenolici (cinnamaldeide, cuminaldeide, eugenolo, alcol cuminico, m-cresolo), e germacrone[91] (5.8%). Secondo Burfield[92] i sesquiterpeni, ed in particolare i derivati furanoidi[93], sono icomposti più importanti per l’aroma caratteristico della mirra: furanoeudesma-1,3-diene, lindestrene, curzerenone, curzerene, cadinene, diidropirocurzerenone. Il germacrone impartirebbe l’odore caratteristico, con note erbacee.
2. Frazione non volatile liposolubile o resina (20%, massimo 40%): acidi alfa-, beta- e gamma-commiforico, acido commiforinico, eeraboresene, alfa- e beta-eerabomirroli e commiferina, campesterolo, beta-sitosterolo, alfa-amirone, 3-epi-alfa-amirina.
3. Frazione non volatile idrosolubile o gomma (30–60%): composti che una volta idrolizzati danno D-galattosio, 4-O-metilglucoronato, L-arabinosio in rapporto 8:7:2[94]. Presente anche dello xilosio.

Utilizzi
Bruciata fin dall’antichità come incenso in Arabia, Somalia ed Etiopia[96]. Morton (1977) riporta che il fumo della resina bruciata veniva usato in caso di febbri e per altri disturbi[97].
Una delle droghe vegetali più antiche e apprezzate, la mirra viene ancora usata a livello popolare, per esempio in Marocco come balsamo per disturbi nervosi e applicata durante le cerimonie di pulizia come fumigazione[98]. Viene usata in Egitto come masticatorio in caso di tosse[99]. Nel mondo arabo si usa come antinfiammatorio, antipiretico, antisettico, e stimolante, ed è un rimedio per gastropatie, indigestione, tosse, asma, bronchite, dolore artritico, lebbra e sifilide.
Mrs Grieve[100] la considera un astringente, vulnerario, tonico e stimolante. Lo consiglia come emmenagogo e come tonico in caso di dispepsia, come espettorante in mancanza di segni di febbre, uno stimolante delle mucose, come carminativo stomachico che eccita l’appetito e il flusso di succhi gastrici e come lavaggio astringente.
Tra gli utilizzi che cita troviamo catarro cronico, tisi, clorosi, amenorrea (con Aloe), gengivite, faringite, afta, ulcere indolenti. Esternamente può essere usata per il suo effetto rubefacente.
Secondo Felter[101], la mirra è la miglior applicazione locale per gengiviti, faringiti con afte e ulcere indolenti, faringite cronica con membrane pallide e umide, tonsillite. Internamente, secondo l’autore, la mirra è uno stimolante delle mucose e non dovrebbe essere usata in condizioni infiammatorie. Piccole dosi promuoverebbero la digestione e sarebbero antisettiche, ma dosi più elevate aumentano il ritmo cardiaco e la temperatura e sono irritanti per le mucose gastriche. E’ comunque un rimedio per soggetti debilitati e condizioni croniche e atoniche, soprattutto per quanto riguarda i polmoni.
Secondo la MTC è una pianta amara e neutrale, che rafforza il sangue e riduce il dolore, riduce il gonfiore e promuove la guarigione delle ferite. E’ una pianta con azioni e indicazioni del tutto simili alla Boswellia (incenso) ed insieme ad essa viene usata per trattare i dolori derivanti da traumi e gonfiori[102]: 1. dolore causato da stagnazione del sangue (dismenorrea; mal di stomaco; dolori articolari da vento-freddo-umido; traumi; dolore da foruncoli e eruzioni); 2. foruncoli e ulcere (esternamente).
Al giorno d’oggi viene occasionalmente utilizzata internamente come carminativo, per problemi di stomaco e come espettorante, ma è usata soprattutto come astringente ed antisettico locale per disordini delle mucose orofaringee e della pelle.
Gli Arabi spalmano la resina su una tela nera che, dopo essersi indurita, viene usata per assicurare le fratture. Gli Indiani dissolvono la mirra in latte di asino o di donna e ne fanno uso come collirio; la somministrano alla donna che allatta per aumentare il flusso di latte; la mescolano con borace in caso di stomatite parassitica; mescolano la tintura di mirra con glicerina in caso di difteria; e la consigliano in forma di tintura in caso di clorosi e dismenorrea in giovani donne. In Dhofar la resina dispersa in acqua viene bevuta o spalmata sul corpo in caso di febbre. In Libano la mirra viene usata come carminativo, fumigatorio, vulnerario, gastrite e influenza. Il fumo viene diretto sulle ferite per favorire la guarigione. In Oman la mirra calda viene applicata alle carie in caso di mal di denti. In Arabia saudita la resina viene applicata al seno delle madri che allattano per svezzare i bambini. In Yemen la resina viene spalmata su morsi di serpente e ferite per guarirle, e sul pene come afrodisiaco[95].
Moore[103] la considera una pianta stimolante per tutti i sistemi. E particolarmente per il fegato, il sistema respiratorio, cardiovascolare, linfatico, riproduttivo e per le mucose. Ha una azione tonica sul sistema nervoso centrale e sul parasimpatico.
I prodotti a base di Mirra sono spesso stati usati a livello topico per problemi di igiene orale, una soluzione ottenuta mescolando e scuotendo fortemente la gommoresina in acqua viene usata per disinfettare le gengive, per le infiammazioni della mucosa orale e faringea e per le afte orali. L’olio di mirra è stato usato nei dentifrici. Altre applicazioni sono labbra secche, emorroidi, ferite ed abrasioni, foruncolosi, alitosi.
Resinoidi ed assolute di Mirra sono usate principalmente in fragranze orientali per impartire una nota balsamica, dolce e resinosa. Il resinoide viene usato anche in fragranze da incenso e basi di ambra dolce. Alcuni autori dichiarano che l’odore della mirra somiglierebbe a quello della traspirazione umana, ma altri autori non ritrovano un carattere fortemente animalico o sessuale.
Farmacologia
Dati sperimentali: la resina è antiossidante (scavenger dei radicali liberi), tireotropica, inibitrice delle prostaglandine, e protegge da vari agenti necrotizzanti, citotossici in topi.
Nella sperimentazione animale la resina, l’olio essenziale e i triterpeni hanno mostrato effetti antimicrobici[104]; l’estratto grezzo della gommoresina mostra attività in vitro di potenziamento dell’attività della ciprofloxacina e della tetraciclina contro S. aureus (anche resistente ai farmaci), molte varietà diSalmonella enterica e di Typhimurium e due ceppi di K. pneumoniae[105].
Altre attività provate in vitro o in vivo su modelli animali sono quelle deodorant[106]e, anti-infiammatori[107]a, antitumor[108]ale, astringente, antipiretic[109]a, ipoglicemizzant[110]e, e protettiva dalle ulcer[111]e gastriche.
La resina sembra stimolare la muscolatura liscia[112] e forse la peristalsi[113]. Stimola il tono uterino[114] e promuove il flusso ematico uterino[115].
I sesquiterpeni furanoeudesma-1,3-dieni e curzarene sono analgesici in vi[116]vosu modelli animali (bloccati da naxolone), con meccanismo forse mediato da recettori oppioidi (una spiegazione del Vinum murratum offerto a Gesù per le proprietà analgesiche?)
Cautele
In mancanza di dati completi, si sconsiglia l’utilizzo della resina di mirra in gravidanza, in allattamento e a bambini, a meno di una specifica indicazione di un professionista[117].
Dosaggio
- Tintura di Mirra (1:5; 90% etanolo)
- Topico
- Tintura pura al bisogno sulla pelle o sulle mucose orali 2-3 volte al giorno
- Colluttorio: 5–10 gocce in un bicchiere di acqua per una azione blanda, fino a 60 per attività più drastiche.
- Dentifricio in polvere: 10% di gommo-resina polverizzata.
<<<<>>>>
[82] Secondo alcuni autori Commiphora molmol era diversa dalla mirra (veniva anche chiamata mirra africana) ma l’odore del fumo era simile e per questa ragione veniva venduta come mirra. Cfr. Tucker, A. O. 1986. Frankincense and myrrh. Economic Botany 40 (4): 425–433
[83] Burfield T. Natural aromatic material – odours & origins. The Atlantic Institute of Aromatherapy, 2000
[84] Bowen, M.R. 1990. A bibliography of forestry in Somalia and Djibuti. Edition two. Natural Resources Institute for Overseas Development Administration, UK and National Range Agency, Somalia. Somali Forestry Papers No. 3
[85] Farmacopea Ufficiale del Regno d’Italia, VI edizione , 1940, Roma
[86] WHO (1999) WHO monographs on selected medicinal plants Vol 3 World Health Organization, Geneva)
[87] Tucker, A. O. 1986. Op. Cit. Langenhein J.H. (2003) Op. Cit.
[88] Arctander, S (1994) Perfume and Flavor Materials of Natural Origin. Allured Publishing Corporation
[89] Burfield T. 2000 Op. Cit.
[90] Farmacopea Ufficiale del Regno d’Italia, Op. Cit.
[91] Brieskorn CH e Noble P (1982) “Unhaltstoffe des eterischen ols de Myrrhe II. Sesquiterpene & Furanosesquiterpene” Medica 44, 87; Olhoff G. (1990) Scents & Fragrances Springer-Verlag pp132-188. Marongiu, Bruno, Alessandra Piras, Silvia Porcedda, and Andrea Scorciapino. “Chemical Composition of the Essential Oil and Supercritical CO2 Extract of Commiphora Myrrha (Nees) Engl. and of Acorus Calamus L.” Journal of Agricultural and Food Chemistry, 2005; Rahman, M , Mark Garvey, Laura Piddock, and Simon Gibbons. “Antibacterial Terpenes from the Oleo-resin of Commiphora Molmol (Engl.).” Phytotherapy Research : PTR, 2008. Hanus LO, Rezanka T, Dembitsky VM, Moussaieff A (2005) Myrrh – Commiphora chemistry. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2005, 149(1):3-28; Zhu, N, H Kikuzaki, S Sheng, S Sang, M Rafi, M Wang, N Nakatani, R DiPaola, R Rosen, and C Ho. “Furanosesquiterpenoids of Commiphora Myrrha.” Journal of Natural Products, 1, 2001
[92] Burfield T. 2000 Op. Cit.
[93] Brieskorn CH e Noble P (1982) Op. Cit.
[94] Hanus LO, Rezanka T, Dembitsky VM, Moussaieff A (2005) Myrrh – Commiphora chemistry. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2005, 149(1):3-28
[95] Duke, J.A., (2008) Op. Cit.
[96] Uphof, J. C. T. 1968. Dictionary of economic plants. New York: Verlag von J. Cramer.; Usher, G. 1974. A dictionary of plants used by man. New York: Hafner Press.
[97] Lemenih, M., T. Abebe, and M. Olsson. 2003. Gum and resin resources from some Acacia, Boswelli and Commiphora species and their economic contributions in Liban, south-east Ethiopia. Journal of Arid Environments 55 (3): 465–482.
[98] Bellakhdar, J.J. 1997. La pharmacopoée marocaine traditionelle. Médecine Arabe ancienne et savouirs populaires. Ibis Press: Paris.
[99] Sameh F. AbouZid Abdelhalim A. Mohamed (2011) Survey on medicinal plants and spices used in Beni-Sueif, Upper Egypt Journal of Ethnobiology and Ethnomedicine, 7:18
[100] Grieve, M (1971, repr. 1931) 1971 A modern herbal; the medicinal, culinary, cosmetic and economic properties, cultivation and folk-lore of herbs, grasses, New York, Dover Publications
[101] Felter, HW (1922) The Eclectic Materia Medica, Pharmacology and Therapeutics. Eclecdtics Publications, USA
[102] Miller JM, Goodell HB. (1968) Frankincense and myrrh. Surg Gynecol Obstet Aug; 127(2):360–5. Greene DA. (1993) Gold, frankincense, myrrh, and medicine. N C Med J Dec; 54(12):620–2
[103] http://www.swsbm.com/ManualsMM/MatMed5.pdf
[104] Newall CA, Anderson LA, Philpson JD. Herbal Medicine: A Guide for Healthcare Professionals. London, UK: The Pharmaceutical Press, 1996. The Review of Natural Products by Facts and Comparisons. St. Louis, MO: Wolters Kluwer Co., 1999
[105] Rahman, M , Mark Garvey, Laura Piddock, and Simon Gibbons. “Antibacterial Terpenes from the Oleo-resin of Commiphora Molmol (Engl.).” Phytotherapy Research : PTR, October 1, 2008. http://dx.doi.org/10.1002/ptr.2501.
[106] Wichtl MW. Herbal Drugs and Phytopharmaceuticals. Ed. N.M. Bisset. Stuttgart: Medpharm GmbH Scientific Publishers, 1994.
[107] Duwiejua M, Zeitlin IJ, Waterman PG, Chapman J, Mhango GJ, Provan GJ. Anti-inflammatory activity of resins from some species of the plant family Burseraceae. Planta Medica, 1993, 59:12–16. Atta AH, Alkofahi A. Anti-nociceptive and anti-inflammatory effects of some Jordanian medicinal plant extracts. Journal of Ethnopharmacology, 1998, 60:117–124. Tariq M, Ageel AM, Al-Yahya MA, Mossa JS, Al-Said MS, Parmar NS. Anti-inflammatory activity of Commiphora molmol. Agents and Actions, 1985, 17:381–382.
[108] al-Harbi MM, Qureshi S, Raza M, Ahmed MM, Giangreco AB, Shah AH.(1994) Anticarcinogenic effect of Commiphora molmol on solid tumors induced by Ehrlich carcinoma cells in mice. Chemotherapy 1994:40:337-47. Qureshi S, al-Harbi MM, Ahmed MM, Raza M, Giangreco AB, Shah AH. (1993) Evaluation of the genotoxic, cytotoxic, and antitumor properties of Commiphora molmol using normal and Ehrlich ascites carcinoma cell-bearing Swiss albino mice. Cancer Chemother Pharmacol. ;33(2):130-8.
[109] Tariq M et al. Anti-inflammatory activity of Commiphora molmol. Agents and Actions, 1985, 17:381–382. Mohsin A et al. Analgesic, antipyretic activity and phytochemical screening of some plants used in traditional Arab system of medicine. Fitoterapia, 1989, 60:174–177.
- [110] Al-Awadi FM, Gumaa KA. Studies on the activity of individual plants of an antidiabetic plant mixture. Acta Diabetologica Latina, 1987, 24:37–41.
- Ubillas RP et al. Antihyperglycemic furanosesquiterpenes from Commiphora myrrha. Planta Medica, 1999, 65:778–779
- [111] al-Harbi MM, Qureshi S, Raza M, et al. Gastric antiulcer and cytoprotective effect of Commiphora molmol in rats. J Ethnopharmacol 1997;55:141-50
- [112] The Review of Natural Products by Facts and Comparisons. St. Louis, MO: Wolters Kluwer Co., 1999. McGuffin M, Hobbs C, Upton R, Goldberg A, eds. American Herbal Products Association’s Botanical Safety Handbook. Boca Raton, FL: CRC Press, LLC 1997
[113] The Review of Natural Products by Facts and Comparisons. St. Louis, MO: Wolters Kluwer Co., 1999.
[114] McGuffin M, Hobbs C, Upton R, Goldberg A, 1997 Op. Cit.
[115] McGuffin M, Hobbs C, Upton R, Goldberg A, 1997 Op. Cit. Brinker F. Herb Contraindications and Drug Interactions. 2nd ed. Sandy, OR: Eclectic Medical Publications, 1998
[116] Dolara P et al. Characterization of the action of central opioid receptors of furaneudesma-1,3-diene, a sesquiterpene extracted from myrrh. Phytotherapy Research, 1996, 10:S81–S83. Atta AH, Alkofahi A. Anti-nociceptive and anti-inflammatory effects of some Jordanian medicinal plant extracts. Journal of Ethnopharmacology, 1998, 60:117–124
[117] British herbal pharmacopoeia. Exeter, British Herbal Medicine Association, 1996. Saha JC, Savini EC, Kasinathan S. Ecbolic properties of Indian medicinal plants. Part I. Indian Journal of Medical Research, 1961, 49:130–151. Pernet R. Phytochimie des Burseraceae. [Phytochemistry of the Burseraceae.] Lloydia, 1972, 35:280–287.
Tutti i tuoi vestimenti sanno di mirra, d’aloe, di cassia
Mirra
“Tutti i tuoi vestimenti sanno di mirra, d’aloe, di cassia;.” Salmi 45:8.
“… sei mesi per profumarsi con olio di mirra e sei mesi con aromi e altri cosmetici usati dalle donne…” Esther 2
Introduzione
Le 150-220 specie[1] appartenenti al genere Commiphora Jacq. (famiglia delle Burseraceae) sono native dell’Arabia meridionale (Oman, Yemen, isola di Socotra), dell’Africa Nord Orientale (52 specie in Somalia, alcune delle quali presenti anche in Etiopia e Sudan), e del Madagascar, ma alcune specie sono native dello Sri Lanka e altre possono crescere anche in India. Due specie meno importanti si trovano anche in Centro America[2]. Si tratta in genere di piccoli alberi dall’habitus arbustivo, spesso usati come palizzate vivente. La loro importanza nella storia dell’uomo deriva però dall’essudato gommo-resinoso da esse ottenuto, usato sin dall’Antichità come rimedio medicinale e come incenso[3]. Le gommo-resine derivanti dalle varie specie di Commiphora (e in senso più generale dalle specie appartenenti alla famiglia delle Burseraceae) mostrano tra loro una forte somiglianza fitochimica e simili applicazioni sia terapeutiche sia rituali, magico-religiose. Si tratta sempre di resine caratterizzate dalla presenza di composti terpenoidici e di intrusioni di polisaccaridi (per cui vengono classificate come gommo-resine, in alcuni testi come oleo-gommo-resine). In effetti questa somiglianza è stata riconosciuta sin dall’antichità, se già i trattati medici della tradizione Sanscrita consideravano le diverse resine come intercambiabili[4].

Quale specie?
A causa di una tassonomia non perfettamente chiarita, e delle ambiguità intrinseche nelle fonti storiche, non è possibile identificare con precisione l’entità tassonomica che corrisponde al materiale resinoso Mirra. Se facciamo riferimento alle citazioni bibliche, Duke[5] argomenta che è impossibile indicare con chiarezza la specie citata nella Bibbia, ma restringe il campo a tre specie, la C. africana (A.Rich.) Engl. (chiamata anche Bdellio o Mirra africana), la C. habessinica (O.Berg.) Engl. e la C. myrrha (Nees) Engl. (detta anche olio di Mirra o Stacte, o Mirra harobol[6]), tendendo a preferire come candidata la C. habessinicasulla scorta dell’opinione di un eminente botanico biblista come Zohary[7] . A testimonianza dell’intrico tassonomico e storico, lo stesso Duke aveva, in un testo precedente, identificato la Mirra con la C. myrrha, e denominato Bdellio la C. africana[8], e in un altro testo aveva invece deciso che il candidato più probabile per la Mirra biblica fosse la C. erythraea[9] Engl. (lo Bdellio profumato o Mirra profumata dell’Antichità, detta anche Opopanax o Mirra bisabol, famosa per il suo profumo estremamente persistente).
Altri autori argomentano che C. myrrha sarebbe la fonte della Mirra del periodo Classico, e non della Bibbia[10], che deriverebbe, come detto sopra, da C. habessinica oppure da C. guidotii Chiov. ex Guid (detta anche Mirra profumata).
In realtà anche al giorno d’oggi la Mirra si ottiene da più di una specie botanica. Nella discussione che segue parleremo di Mirra in senso generico per intendere la droga storicamente riconosciuta, a prescindere dall’esatta fonte botanica, e solo nell’ultima parte dell’articolo ci soffermeremo sulle caratteristiche specifiche della specie paradigmatica.

Storia
Il termine italiano Mirra traduce una parola latina (Myrrha, o Murrha, o Murra) derivante dalla parola Greca múrrā, a sua volta di origine semitica, con radici nell’Arabo murr, nell’Ebraico mōr e nell’Aramaico mūrā, tutte con lo stesso significato, amaro (il termine Smyrna è una forma dialettale greca derivante da Myrrha). Questo termine identifica la resina aromatica prodotta da specie diCommiphora che crescono in Arabia e in Africa orientale subtropicale, usata dagli antichi come profumo[11], per imbalsamare[12] (tanatoprassi, taxidermia), come anodino[13], e per molte altre applicazioni (vedi più sotto le Indicazioni storiche). In Antichità venivano riconosciute due varietà di mirra: la bissa bol(Bhesabol/Bysabole/Hebbakhade in Somalia), e la Mirra Araba, coltivata con Acacia, Moringa ed Euphorbia. In realtà il termine Myrrha non identificava necessariamente una specie del genere Commiphora, ma serviva a denotare qualsiasi pianta profumata; infatti una seconda traduzione dell’ebraico mor fa riferimento alla parola ebraicalot, che porta a Ladanum/Labdanum, la resina del Cistus ladanifer L. (Cistaceae).
Il più antico resoconto scritto sugli usi etnomedici della Mirra proviene dalla Mesopotamia e risale al 2.600 a.C.; in esso si descrive l’uso di migliaia di derivati dalle piante, tra i quali troviamo anche le resine/olii di Cedrus sp., di Cupressus sempevirens L. ed anche di Mirra14], usate in casi di infiammazione.
In tutta l’Asia minore era comune il suo utilizzo per riti funerari, per ungere il capo ed il corpo delle persone, per imbalsamare i morti (il termine imbalsamare viene da in balsamum, conservare con un balsamo, termine generico che identificava qualsiasi resina abbastanza fluida[15]).
La Mirra era certamente conosciuta nell’Egitto antico, probabilmente fin dal III millennio a.C., periodo per il quale si hanno notizie dell’utilizzo di molte sostanze aromatiche per il rito dell’imbalsamazione – una volta che il corpo era stato essiccato immergendolo nella sabbia del deserto, è possibile che venisse unto con resine o olii derivati da legno di cedro, ginepro, cannella, chiodi di garofano e noce moscata, ma soprattutto con le resine di tre specie di Commiphora: Mirra, Balsamo (Commiphora opobalsamum Engl.) e Bdellium (Commiphora mukul[16] (Hook. ex Stocks) Engl.).
Vasi ritrovati nella tomba di Tutankhamen (1.350 a.C., aperta nel 1.922 d.C.) contenevano ancora tracce d’incenso e mirra e altre piante aromatiche. Le indagini hanno chiarito che la resina fu usata nella camera mortuaria sia come agente mummificante, sia come vernice, cemento e materiale per ornamento personale[17] del faraone.
Papiri risalenti al 2.800 a.C. (regno di Khufu) riportano usi magici/medicinali di sostanze aromatiche. I dolori muscolari erano trattati con unguenti contenenti incenso e cannella; per le malattie della pelle (forse herpes) gli unguenti utilizzati contenevano mirra, coriandolo e miele.
Secondo i documenti, in Egitto l’uso religioso dei materiali aromatici era ben strutturato: al mattino venivano bruciate delle resine, a mezzogiorno della mirra, mentre al tramonto il dio Ra veniva venerato con offerte della miscela detta Kyphi (preparazione particolarmente famosa che, secondo fonti più tarde, conteneva sedici ingredienti tra i quali materiali nativi come il ginepro, menta piperita, uva passa,ed altre piante aromatiche, mescolati a miele e vino, e materiali esotici comeincenso, mirra, e cannella[18]), utilizzata dai sacerdoti come mezzo per “trasportare” il dono dell’uomo verso gli dei. Il Kyphi non aveva solo utilizzi religiosi, serviva anche per facilitare il sonno, alleviare le ansie, aumentare i sogni, eliminare la tristezza, trattare l’asma ed agire come un antidoto generico.
Secondo Hoots[19] inizia in questo periodo il commercio su scala significativa della Mirra, proprio perché era ampiamente utilizzata come incenso nei templi, come profumazione delle mummie ed in altre applicazioni, grandi erano le quantità necessarie (alcune iscrizioni nel 2.500 a.C. parlano di 80.000 misure di mirra[20]), e in Egitto non era possibile coltivare l’albero.

La prima testimonianza scritta chiara sull’uso significativo di resine esotiche in Egitto risale però al 15°secolo a.C, è relativa al suo trasporto commerciale[21], ed è contenuta in una iscrizione del tempio dedicato alla Regina Hatshepsut di Tebe. Dalle iscrizioni si legge come essa ordinò una spedizione verso il Mar Rosso, perraccogliere incenso delle terre di Punt (una zona non ben delimitata forse comprendente la costa della Somalia e una porzione della costa Araba opposta, alla bocca del mar Rosso). In quella che è stata descritta come la prima spedizione di raccolta di piante/etnobotanica, trentun alberi di incenso furono riportati indietro e piantati presso il tempio di Karnak sulle rive del Nilo superiore. Non è in realtà chiaro se si trattasse veramente di alberi di Boswellia, ed è più plausibile che si trattasse di alberi di Commiphora myrrha, dato che essa è una delle specie tipiche della Somalia.


L’antico Egitto si pose quindi come intermediario tra il Mediterraneo ed i mercanti Arabi nell’attuale Yemen, i quali a loro volta commerciavano con l’India.
Erodoto[22] nel V secolo a.C. nota l’importante ruolo della mirra per il processo di imbalsamazione in Egitto, e lo spiega raccontando una leggenda: si racconta che ogni 500 anni la fenice rinata depositasse un contenitore a forma di uovo e fatto di pura resina di mirra, racchiudesse il corpo del suo padre appena deceduto all’interno dell’uovo e lo portasse dall’Arabia in Egitto perché fosse cremato presso il tempio di Ra ad Heliopolis[23].
La resina era anche conosciuta in Israele e in Assiria dove il re Assurnasirpal II (883-859 a.C.) aveva trapiantato un albero di Mirra nei suoi giardini botanici presso Calah (la moderna Nimrud, antica città Assira a sud di Mosul nell’Iraq del Nord).
Nelle antiche pratiche giudaiche Greche e Romane la mirra veniva usata per il culto degli dei ma anche in molte occasioni sociali, pubbliche e private. Era associata all’intimità del piacere sensuale. Saffo[24] nel VI secolo a.C. parla delle volute di fumo di mirra, cassia e incenso durante un matrimonio.
La mirra (insieme all’incenso) è naturalmente molto presente negli scritti biblici, ci sono ventidue citazioni delle due resine tra il Vecchio e il Nuovo Testamento[25]. Il Vecchio testamento parla di unguenti medicamentosi a base di mirra, cannella, cassia, calamo aromatico, ecc., e la mirra era l’ingrediente principale dell’olio sacramentale degli ebrei nel Vecchio Testamento[26], e Gesù rifiutò “vino mescolato a mirra” (Vinum murratum) durante la crocifissione[27] facendo si che la Mirra fosse associata al suo martirio (mentre l’Incenso è associato alla sua divinità).
Anche nei testi biblici è presente l’associazione con l’intimità del piacere sensuale: nel libro ebraico dei Proverbi una adultera dice: “Ho guarnito il mio letto di morbidi tappeti, di coperte ricamate con filo d’Egitto/ l’ho profumato di mirra, d’aloe e di cinnamomo./Vieni inebriamoci d’amore fino al mattino, sollazziamoci in amorosi piaceri;” (Proverbi 7:16-18).
Viene anche citata varie volte nel Cantico dei Cantici: “… Sono entrato nel mio giardino, o mia sorella, sposa mia, ho colto la mia mirra col mio balsamo; ho mangiato il mio favo col mio miele, ho bevuto il mio vino col mio latte. Amici, mangiate, bevete; sì inebriatevi, o diletti…” (Cantico dei cantici 5:1); “L’amico mio ha passato la mano per il buco della porta, e le mie viscere si son commosse per lui. Mi son levata per aprire al mio amico, e le mie mani hanno stillato mirra, le mie dita mirra liquida, sulla maniglia della serratura” (Cantico dei Cantici 5:4-5).
Viene citata nella genesi: “Allora Israele, loro padre, disse loro: “Se così è fate questo: Prendete ne’ vostri sacchi delle cose più squisite di questo paese, e portate a quell’uomo un dono: un po’ di balsamo, un po’ di miele, degli aromi e della mirra, de’ pistacchi e delle mandorle.” (Genesi 43: 11), nell’Esodo: “Procurati balsami pregiati: mirra vergine per il peso di cinquecento sicli, cinnamòmo odorifero, la metà, cioè duecentocinquanta sicli, canna odorifera, duecentocinquanta” (Esodo 30:23) e nei Vangeli; Giovanni parla della sepoltura del Cristo: “Vi andò anche Nicodèmo, quello che in precedenza era andato da lui di notte, e portò una mistura di mirra e di aloe di circa cento libbre./ Essi presero allora il corpo di Gesù, e lo avvolsero in bende insieme con oli aromatici, com’è usanza seppellire per i Giudei.” (Giovanni 19: 39-40), e nel Vangelo secondo Matteo la mirra è uno dei doni portati dai Re Magi a Gesù Bambino (Matteo 2:11).
Con il nome Myrrha o Smyrna era conosciuta dai greci nel VI secolo a.C. e in seguito Teofrasto (322-287 a.C.) fu in grado di dire qualcosa delle sue origini grazie alle notizie derivanti dalla spedizione di Alessandro il Grande in Arabia[28]. Nella Historia Plantarum egli parla di Stacte o Mirra liquida, e ne descrive l’utilizzo per speziare i vini. Era molto usata anche in medicina, anche se il giudizio su quale fosse la miglior qualità differisce secondo gli autori: Teofrasto[29] preferisce quella invecchiata mentre Dioscoride[30] dichiara che la migliore è quella più fresca, leggera e friabile, perché più pungente e riscaldante.
Strabone (64-24 a.C.) nel suo Geografia cita il regno di Saba (la Sabaea – attuale Yemen) come fonte di balsamo, cannella, incenso e mirra.
Nel Corpus Hippocraticus è la resina citata più spesso, per ben cinquantaquattro volte, spesso per disturbi legati agli epiteli: in “De Fistulis” si consiglia di usarla per trattare fistole anali[31], in “De haemorrhoidibus ” viene usato per curare le emorroidi al posto della cauterizzazione o dell’incisione[32], e in De Ulceribus viene descritto un lungo procedimento per la produzione di un linimento secco a base di mirra ed incenso da applicare su ulcere e piaghe, vecchie e nuove[33].
Dioscoride usa la mirra in una ricetta per il mal d’orecchi, dove l’ingrediente principale è il latice del papavero da oppio (Papaver somniferum L.), mescolato a mirra, olio di mandorle e zafferano[34].
Ma sono le fonti romane, in particolare Plinio il Vecchio, che dominano la letteratura sulla mirra. Intorno al primo secolo a.C., è infatti questo autore nella sua Naturalis Historia a raccogliere la maggior messe di dati sull’argomento[35], e a dare molti dettagli sulla pianta, sulle sue origini e sulla raccolta, e sulle sue qualità “riscaldanti, mordenti, astringenti e leggermente amare[36]“.
Ci dice Plinio che:
L’albero che produce la Mirra viene allo stesso modo inciso due volte all’anno, nella stessa stagione dell’albero dell’Incenso, ma nel suo caso le incisioni vengono effettuate a partire dalle radici su fino ai rami forti a sufficienza. Prima di essere inciso, l’albero essuda un succo chiamato Stacte, che è la più apprezzata di tutte le Mirre. Subito dopo di questa viene il tipo coltivato, ed anche la miglior qualità del tipo selvatico, quella raccolta in estate.
In tutta la regione viene raccolta e trasportata da persone ordinarie e messa in sacchi di cuoio. I nostri profumieri non hanno difficoltà a distinguere i differenti gradi, grazie all’evidenza dell’aroma e della consistenza. Vi è un gran numero di varietà (…). Parlando in generale, comunque, la mirra è di buona qualità se è costituita da piccoli pezzi di forma irregolare, che si formano al solidificarsi e allo sbiancarsi del succo nel momento in cui si secca; ed anche se mostra segni bianchi, come unghie quando viene rotta, e ha un sapore leggermente amaro[37].
La sua introduzione nei riti religiosi è testimoniata da molti autori classici[38], e diventa anche protagonista di racconti mitici. Rifacendosi allo schema di un mito narrato dallo Pseudo-Apollodoro nella Bibliotheca, Ovidio, nelle sue Metamorfosi (ma il mito, con variazioni, è raccontato anche nelle Fabulae di Igino, e nelle Metamorphoses di Antonino Liberale), racconta della nascita dell’albero di mirra. Myrrha, la figlia del re di Cipro, Cinira, e di Cencreide, desiderava incestuosamente il padre[39].
Con l’aiuto della nutrice riuscì ad ingannare il padre per giacere con lui per varie notti, ma venne scoperta e, incinta, fuggì per salvarsi dall’ira del padre. Arrivata alla città di Saba e pronta a partorire, Myrrha confessa le sue colpe agli dei e chiede di essere bandita sia dal mondo dei vivi che da quello dei morti. Gli dei ascoltano la sua preghiera e la trasformano in un albero che stilla gocce di pianto profumato dalla corteccia. Adone, aiutato da Giunone Lucina (“colei che porta i bambini alla luce”), riuscirà a nascere dal grembo legnoso.

La mirra è uno degli ingredienti principali della farmacopea romana con più di 200 citazioni, ed anche se non aveva la popolarità dell’Incenso, il suo prezzo era di molto superiore e per questo divenne un simbolo di status sociale ed economico, oltre che simbolo religioso e strumento terapeutico.
La mirra era una componente principale di un vino speziato molto apprezzato dai Romani, il Musulm, un aperitivo contenente forse miele, vino, radici di Sausurrea costus (Falc.) Lipsch, e Cinnamomum tamala (Buch.-Ham.) T.Nees & Eberm., oppure, secondo un’altra versione, Mirra, Cinnamomum aromaticum Nees., Sausurrea,Nardostachys jatamansi (D.Don) D.C., Pepe e Miele[40].
Le rotte commerciali
Dal 2.000 a.C. gli Arabi monopolizzano il mercato, per il momento ridotto e locale, di Boswellia e Commiphora, mercato che vedrà una prima forte accelerazione grazie alla introduzione del cammello in Arabia del Sud, domesticato nel 2.000 a.C. ma divenuto importante mezzo di trasporto solo intorno al 1.000 a.C. Questo animale velocizzerà enormemente il trasporto via terra, e permetterà di raggiungere le aree del Mediterraneo più lontane, in tempi più brevi e con carichi molto maggiori, e permetterà quindi l’incontro tra domanda e offerta in maniera più efficace. La domanda era dominata prima da Greci e in seguito Romani, che utilizzavano ampiamente gli incensi per doni e offerte agli dei, per nutrirli con l’unico cibo che l’uomo poteva offrirgli (cfr. lo stesso utilizzo dell’incenso come cibo per gli dei che si riscontra in America tra i Maya).
È proprio in questo periodo che il mercato delle spezie diventa economicamente molto importante per le terre Arabe, e questo successo commerciale raggiunge l’apice intorno al 750-500 a.C., creando la ricchezza delle terre arabe. Si hanno di questo periodo testimonianze dell’uso delle spezie per unguenti e incensi in Palestina.
E così l’aumentare dell’importanza commerciale delle resine delle due piante porta allo stabilirsi di tratte commerciali via terra sempre più stabili, all’aumentare in numero e frequenza delle carovane e quindi al crescere di agglomerati urbani intorno alle stazioni di scambio e di riposo per le stesse.
Al crescere dell’importanza delle rotte, del volume di incenso e della sicurezza rispetto ai banditi, altre merci iniziarono as essere trasportate, come ad esempio le spezie, l’avorio e la seta dall’India, e oro, legni e pellami preziosi dalla costa africana. La stessa carovana riportavano beni manifatturieri dall’Etruria, della Grecia e da Roma, aumentando la ricchezza o l’importanza dei centri commerciali in Arabia.
Questo attivo interscambio favorì la nascita delle prime città-stato dell’area araba, la più famosa delle quali è probabilmente Saba (la Sabaea). Si narra che nel 992 a.C. la Regina di Saba portò delle spezie in dono a Re Salomone, e che la città raggiunse una tale ricchezza da poter costruire delle dighe e opere d’irrigazione e canalizzazione per migliorare l’irrigazione delle sue terre, rendere più ricca e produttiva l’agricoltura[41]. Una grande diga costruita nell’8 secolo a.C. serviva ad irrigare gli orti e i giardini della capitale Mar’ib, così famosi da essere ritenuti il giardino dell’Eden menzionati nella Bibbia e nel Corano. Mar’ib rimase un importante centro anche dopo il 5° secolo aC quando iniziarono ad emergere nuovi stati rivali
Il commercio con l’area Mediterranea crebbe sempre di più, e divenne più organizzata, almeno secondo le testimonianze a noi pervenute. Erodoto parla di un commercio molto importante intorno al 500 a.C., tale che: “tutto il paese è profumato con esse [le resine aromatiche] ed emana un odore meravigliosamente dolce”. Teofrasto, intorno al 300 a.C. racconta della prima testimonianza oculare degli alberi di incenso e della raccolta della resina secondo la relazione delle spedizioni di Alessandro il Grande.
La via dell’Incenso continuò a crescere di importanza nel periodo subito prima la nascita di Cristo, come testimonia la citazione di carovane di 2-3000 cammelli.
Anche se è probabile che esistesse una rotta commerciale preferenziale per l’incenso verso il Mediterraneo, che possiamo chiamare la via dell’incenso, questa aveva comunque molte varianti e alcune deviazioni.
La principale via di commercio era quella che si originava nelle regioni di Dhofar (Oman meridionale), Somalia, e dall’isola di Socotra, da dove le navi cariche di merci partivano per arrivare, dopo 800 km di navigazione, al porto di Qana (odierna al Mukalla) in Yemen. Da qui venivano trasportate per terra fino all’emporio del governatorato di Shabwah dove venivano tassate.
Rotta del Mar Rosso
Da Shabwah esse continuavano per Narib, da dove potevano prendere la via del Mar Rosso, e proseguire fino a Jeddah (dove risalivano i pellegrini provenienti dalla Mecca), Da qui le navi proseguivano verso la penisola del Sinai e Suez, e dopo 2.000 km arrivavano in Palestina, a Petra e al porto di Gaza da dove potevano partire direttamente per il resto del Mediterraneo, oppure continuavano il viaggio via terra verso Alessandria d’Egitto, da dove venivano vendute localmente e in piccole parte spedite verso Roma, Grecia e Spagna (anche se la maggior parte dell’incenso per Roma veniva processato ad Alessandria, che era il centro industriale dell’Impero Romano). Da Alessandria l’incenso faceva altri 2.100 km per mare fino a Roma (6.500 km in totale).
Rotta del Mar Rosso: Nubia-Alto Egitto-Delta del Nilo
Una rotta alternativa, più difficile e pericolosa, partiva da Port Sudan, di fronte a Jeddah. Da qui partiva una rotta desertica e difficile, con poca acqua, pochi punti di ristoro; arrivava ad Assuan, poi a Qus (dove si incontravano i flussi mercantili e dei pellegrini della Mecca), Koptos, Cenopolis, e infine Luxor, dove la mercanzia veniva caricata su barconi per discendere il corso del Nilo fino al Cairo, da dove si arrivava facilmente ad Alessandria e potevano fare scalo al porto di Sudan, di fronte a, e scaricare le merci.
Rotta Iraq-Siria-Palestina
Una via alternativa partiva da Narib per poi piegare verso il Golfo Persico, passare per Gherra (un sito di interscambio per Persia e Mesopotamia) e poi Teradon. Da qui le navi risalivano la corrente fino alla città di Bassora da dove potevano proseguire fino alla città di Bagdad oppure scendere e viaggiare via terra verso Siria ed Egitto.
Tra le vie di terra era considerata la migliore perché attraversava il territorio storico del Califfato d’Oriente, benevolo nei confronti dei commercianti arabi. Il viaggio era intrapreso da carovane di cammelli che si fermavano per ristoro o dormire nei molti caravanserragli distribuiti lungo le piste.
La via di terra iniziava da Bagdad, dopo che le navi che avevano risalito il Tigri avevano scaricato le merci. Il percorso si snodava verso ovest lungo il corso del Tigri, con molti caravanserragli, passava per Samarra, Tikrit, e Mosul, dove abbandonava il corso del fiume per piegare più decisamente ad ovest, entrando in Siria, per spingersi fino ad Aleppo, vicino al porto cristiano di Antochia. Da qui piegava a sud per Hamat, Homs e finalmente Damasco. Le navi, per attraversare il Mediterraneo, potevano partire da Antiochia e Tiro, oppure la carovana si spingeva a Sud, passando per Gerusalemme fino ai porti di Gaza o Alessandria.
Le rotte del Mediterraneo. Costa Nord
Se il cargo partiva da un porto cristiano come Antiochia o altri, allora avrebbe fatto scalo a Cipro, poi a Rodi, a Creta, per arrivare in Sicilia, passare lo stretto di Messina, passare per Cefalù, Palermo e Trapani. Da qui la traversata fino ala Sardegna, proseguendo per Ibiza e la costa andalusa, Denia o Cartagena (dal XIII secolo, dopo la riconquista da parte dei re cristiani di queste città), oppure Malaga.
Litorale magrebino.
Se invece la nave partiva da un porto musulmano, come Alessandria, il viaggio proseguiva in direzione ovest lungo la costa nordafricana passando per Barca, Tripoli, Gabes, Tunisi e Algeri, da dove le navi attraversavano il tratto di mare che le divideva dall’Andalusia, ad Almeria oppure a Malaga.
Altre rotte
Gli incensi non venivano esportati solo verso nord, ma anche verso est, verso l’India e la Cina, insieme ad altre resine come Storace e Sangue di Drago di Socotra. La mirra è presente nella letteratura Sanscrita dal VII secolo a.C. in avanti, mentre arriva in Cina molto più tardi, intorno al V secolo d.C.. Nel XII secolo d.C. Zhao Rugua descrive una mirra proveniente sia dall’Arabia del Sud sia dalla moderna Somalia. Nel 1342 il Kahn del Catay manda a Papa Benedetto XII regali d’oro, argento, seta, perle, canfora, muschio, mirra e spezie[42]. Con tutta probabilità la mirra faceva un viaggio circolare con i commercianti arabi, dalla Persia alla Cina e ritorno.
Per rendersi conto del valore delle resine basti riportare la testimonianza che gli addetti alla lavorazione ad Alessandria venivano denudati e perquisiti perchè non facessero uscire nulla, e l’opinione è che l’incenso valesse più dell’oro, e fosse forse la sostanza più preziosa sulla terra intorno alla nascita di Gesù.
Secondo i calcoli di Plinio, venivano prodotti 2,5-3 milioni di kg di mirra che valeva 3 volte l’incenso (Boswellia) che però era richiesto a volumi fino a cinque volte superiori.
Anche se per molti secoli le civiltà del Mediterraneo non conobbero le aree di produzione e di provenienza degli incensi, al crescere della loro importanza economica e commerciale aumentò l’interesse dei Romani per il mercato delle spezie. Dopo il 27 a.C. (la data esatta è dibattuta[43]) Aelius Gallus, governatore d’Egitto(45 – 5 BCE ), sedotto dalla possibilità di controllare il mercato delle spezie che stava arricchendo il reame alleato di Nabatea, partì con una spedizione forte di 10.000 uomini per i deserti Arabi per trovare gli alberi di incenso. La spedizione fu un insuccesso ed i Romani dovettero ritirarsi, sconfitti dalle malattie, dalla mancanza di acqua e dalla resistenza delle tribù locali.
Per quanto un insuccesso, la spedizione rese possibile pensare alla conquista del commercio degli incensi, che si rese possibile più tardi grazie alla scoperta dei monsoni. Con questa scoperta si rese possibile dimezzare i tempi di viaggio per mare verso l’Arabia e l’India. Quindi nel 2-3° secolo d.C. i mercanti Romani riuscirono a bypassare i mediatori arabi e le tasse che pesavano sugli incensi, contribuendo, intorno al 400 d.C., al declino del commercio dell’incenso e delle città che fiorirono su esso. I flussi di resine dalle terre arabe scemarno fino a terminare, a causa anche della lenta ma continua depauperazione delle popolazioni autoctone di Boswellia e Commiphora nell’odierno Yemen, causata da una cattiva gestione e cura delle piante, da uno sfruttamento distruttivo, alla crescente pressione delle mandrie di animali (cammelli e capre) ghiotti di incenso, oltre ad un concomitante periodo di siccità, fattori che hanno portato alla scomparsa delle piante di Boswellia sacra in buona parte dell’Arabia meridionale.
Responsabile del declino fu però anche l’opposizione della chiesa cristiana. Quando il Cristianesimo divenne religione di stato a Roma, alla fine del 4° secolo, l’imperatore Teodosio I vietò infatti l’uso delle offerte agli dei, e l’utilizzo degli incensi, visti come residui di paganesimo, anche se la chiesa stessa finirà per adottare incenso e mirra qualche secolo più tardi (intorno al 700 d.C.) all’interno della liturgia. In effetti la mirra divenne un ingrediente fondamentale di alcune versioni del Crisma battesimale. Una delle ricette pervenute a noi lo descrive così composto:
- 500 p di mirra +
- 250 p di cannella +
- 250 p di calamo +
- 500 p di Cassia +
- Olio di oliva
Con la perdita di ricchezza conseguente al declino, Il commercio per nave si ridusse al lumicino, le popolazioni dell’area di Saba iniziarono ad abbandonare l’area e a ritirarsi sugli altipiani dello Yemen, e si formò un altro stato centralizzato, Hymar, che si sostituì a Saba nel comandare i porti sul Mar Rosso.
Nel XVI secolo entrarono in voga i “rimedi da indossare” sotto forma di polveri, guanti, collane ed altri oggetti profumati, profumi, ecc., tutti naturalmente caratterizzati da ingredienti esotici tra i quali naturalmente figurava anche la mirra[44].
Indicazioni tradizionali
Secondo gli antichi autori[45] le qualità della mirra erano: calda (calefaciens, fluxiones sistens[46]), risolutiva (“carnes rodunt[47]“, “compositio caustici[48]“, “emollientes[49]“), mordente[50], astringente[51], amara[52], analgesica[53].
Vi sono molti esempi di autori antichi che hanno formulato dei rimedi comprendenti la resina di mirra
Gaio Elio Gallo (45–5 a.C. ), il prefetto romano in Egitto, protagonista della disastrosa spedizione alla conquista dell’Arabia felix, aveva anche interessi medici. Galeno[54] cita una sua teriaca contro le punture degli scorpioni, un multifarmaco che: ” . . .Gallo portò fuori dall’Arabia e diede a Cesare [Augusto], [e] molti soldati furono curati con esso.” Probabilmente Gallo era un Asclepiade, dato che Galeno cita un “Marco” Gallo, discepolo di Asclepio (Esculapio), come inventore di un utile aiuto preventivo (da usare prima di pasti lussuriosi), composto da semi di Giusquiamo, rose, anice, semi di sedano, mirra vecchia e zafferano, bolliti in vino e miele[55].
Gallo inventò anche degli antidoti per la golosità, contenenti mirra ed altre spezie costose ed importate[56]. Galeno cita[57] un testo di Elio Gallo che loda l’utilità di incenso, mirra, le due cannelle ed altri ingredienti esotici nella manifattura di gocce efficaci contro la tosse ed altre medicine utili a lenire le vie aeree.
Claudio Alcimo (Alchimione – 120 a.C.– 25 d.C.), il medico di Tiberio o Claudio viene citato due volte da Galeno[58]. Gli si attribuisce un trattamento emolliente composto da cera d’api, resina di Colofonia, resina di Dorema ammoniacum D.Don, galbano, mirra, incenso, opopanax (Balsamo della Mecca), propolis, aceto, feci di capra, e olio d’oliva[59].
Abascanto di Lugdunum (10 a.C. – 80 d.C.) formula un rimedio per la tisi contenente resina di mirra, Aristolochia spp. (A. clematis L.), zafferano, euforbia, genziana, Hyoscyamus niger L., Mandragora officinarum L., oppio, ecc.[60], un rimedio per le coliche contenente resina di mirra, Nardostachys jatamansi, oppio, pepe, ecc. in vino cotto[61], e un antidoto: resina di mirra, castoreo (sostanza giallognola prodotta dal castoro), zafferano, Iris illyrica[62], oppio, pepe bianco, Teucrium spp. (T. chamaedrys L.), ecc., in vino[63]
Amutaone (120 a.C. – 80 d.C.) preparava unguenti contenenti Bdellio, Incenso e Galbano, in una base di trementina e cera d’api[64]; uno in particolare, che conteneva anche olio di Hennè, resina di Dorema ammoniacum e di mirra, veniva usato per dolori articolari.
Come si capisce dagli esempi sopra riportati, i campi di applicazioni proposti nel tempo per la mirra erano molti:
- Pneumologia: l’indicazione principale della mirra. Tosse e “tracheiti[65]“, asma[66], angina[67], disfonie[68], otiti[69], broncorrea.
- Dermatologia: dopo la penumologia è l’indicazione più comune. Ascessi, impetigine, erisipela, ulcera, “infiammazioni” locali in genere[70].
- Apparato digerente: dolori addominali, “cholera”, “malattie del fegato”, emorroidi, fessure anali[71].
- Ginecologia: mestruazioni irregolari[72]
- Nefrologia: usata come diuretico[73]
- Neurologia: spesso menzionato per il trattamento dei dolori (“acopum ad omnem contractionem nervorum[74]“), in particolare delle cefalee, delle “nevralgie[75]” e dell’opistotono[76]
- Oftalmologia: Galeno “oculorum ulcera et crassas cicatrices[77]“
- Otorinolaringoiatria: instillazioni auriculari[78], e trattamento angina.
- Reumatologia: dolori articolari e podagra[79].
- Stomatologia: presente in varie preparazioni per denti e gengive (“colluta dentes gingivasque[80]“)
- Traumatologia: è il classico vulnerario dell’antichità.
- Tossicologia: secondo Celso e Scribonio Largo la mirra entra a far parte di vari antidoti[81].
Le principali forme galeniche usate in antichità erano tre: resina compatta, semifluida (profumo “in lacrime”, “stakte” greca) o dissolta in vino (vino di mirra o vinum murratum utilizzato per il catarro respiratorio), olio o acqua calda.
Si usava per via interna come diuretico o stimolante, come linimento su piaghe o per dolori reumatici, come pomata oftalmologica, nelle instillazioni auricolari e come compressa di resina applicata sulle fratture.
<<<<>>>>
[1] The Plant List (2013). Version 1.1. Published on the Internet; http://www.theplantlist.org/ (visionata il 21 Gennaio 2014
[2] Mabberley DJ (1987) The Plant-Book. A portable dictionary of the higher plants. Cambridge: Cambridge University Press
[3] Langenhein J.H. (2003) Plant Resins: Chemistry, Evolution, Ecology, and Ethnobotany. Timber Press, Oregon
[4] Langenhein J.H. (2003) Op. Cit.
[5] Duke, J.A., (2008) Duke’s handbook of medicinal plants of the Bible. CRC Press Taylor & Francis, Boca Raton
[6] Fluckiger, F. & Hanbury, D. (1885) Pharmacographia – The History of the Principle Drugs of Vegetable Origin. Reprinted Delhi (1986)
[7] Zohary, M. 1982. Plants of the Bible. Cambridge University Press, New York
[8] Duke, J.A. 1983. Medicinal Plants of the Bible. Trado-Medic Books. A Division of Conch Magazine Ltd
[9] Duke, J.A. 1999. Herbs of the Bible — 2000 Years of Plant Medicine. Interweave Press, Loveland, CO
[10] Langenhein J.H. (2003) Op. Cit.
[11] Esodo 30:23; Salmi 44:9; Proverbi 7:17; Cantico dei Cantici 1:12; 5:5
[12] Giovanni 19:39
[13] Marco, xv, 23
[14] Newman, D.J., Cragg, G.M., Snader, K.M. Nat. Prod. Rep. 2000,17, 215–234
[15] Langenhein J.H. (2003) Op. Cit.
[16] Turner, J (2004) Spice: The history of a temptation. Vintage Books, Random House
[17] Turner, J (2004) Op. Cit.
[18] Dalby, A (2000) Dangerous tastes: The history of spices. University of California Press, Berkeley
[19] Hoots, C. 1993. Retracing the incense route. Mosaic 1993(Feb.): 43–45.
[20] Majino J. 1975 The healing hand: Man and wound in in the ancient world. harvard University Press
[21] Groom, N. 1981. Frankincense and Myrrh: a Study of the Arabian Incense Trade. Longman,New York.
[22] Erodoto H 2.73 in J.P.A. Gould; J.S. Romm, Herodotus (1998); BNP 6 (2005) 265–271, K. Meister; C. Dewald & J. Marincola, The Cambridge companion to Herodotus (2006).
[23] Dalby, A (2000) Op. Cit.
[24] Lobel, E Page, D (1955) Poetaram Lesbiorum Fragmenta, Oxford, Clarendon. 1955; II ediz. 1963, p 44
[25] Duke, J.A., (2008) Op. Cit.
[27] “Gli diedero da bere vino mescolato con fiele. Egli lo assaggiò, ma non ne volle bere. (Mt 27,34)
E subito uno di loro corse a prendere una spugna, la inzuppò di aceto, la fissò su una canna e gli dava da bere. (Mt 27,48) e gli davano vino mescolato con mirra, ma egli non ne prese. (Mc 15,23)
Uno corse a inzuppare di aceto una spugna, la fissò su una canna e gli dava da bere, dicendo: «Aspettate, vediamo se viene Elia a farlo scendere». (Mc 15,36)
Vi era lì un vaso pieno di aceto; posero perciò una spugna, imbevuta di aceto, in cima a una canna e gliela accostarono alla bocca”. (Gv 19,29)
[28] Dalby, A (2000) Op. Cit.
[29] Plinio NH, 12.68-71
[30] Dioscoride MM 1.25
[31] De Fistulis Sez 3 e 5. In CD Adams 1868 The Genuine Works of Hippocrates. Hippocrates. New York. Dover.
[32] De haemorrhoidibus, sez 6. In CD Adams 1868 The Genuine Works of Hippocrates. Hippocrates.. New York. Dover.
[33] De Ulceribus, sez 5. In CD Adams 1868 The Genuine Works of Hippocrates. Hippocrates. New York. Dover.
[34] Scarborough, J. (1995) The opium poppy in hellenistic and roman medicine’ in R Porter and M Teich (eds.) Drugs and narcotics in history. Cambridge, New York: Cambridge University Press.
[35] Plinio NH, 12.68-71
[36] Plinio NH
[37] Plinio NH, 12.68-71
[38] Ovidio, Le metamorfosi, VI, 14. Virgilio, “Eneide”, I, 146
[39] Ovidio, Le metamorfosi, X 298-502
…poi, nascondendo il volto con la veste per la vergogna, sospira: “Beata te, mamma, che l’hai sposato!”. Non dice altro e geme. Un brivido di gelo corre per il corpo della nutrice, che ormai ha capito, fin dentro le ossa, e sul capo le si rizzano i capelli, arruffando tutta la canizie (Ovidio, Le metamorfosi, X.421-425)
[40] Dioscoride MM 1.25, 1.64, 1.64; Plinio NH, 12.68-71; Erodoto H 2.73; Saffo 44 Lobel, E e Page, D (1955) Op. Cit. Proverb 7.17-18; Orazio Odi 3.14.21-4
[41] Langenhein J.H. (2003) Op. Cit.
[42] Yule, H. (1886) Cathay and the Way Thither, Hacklutt Society, London, pp.357
[43] Jameson S. (1968) Chronology of the Campaigns of Aelius Gallus and C. Petronius. JRS 58 71–84
[44] Thompson, CJS (1927) The mistery and lure of perfume, London, pp-99-163; Matthews, LG (1973) The antiques of perfume London, pp.10-16
[45] Cfr. Keyser PT, Irby-Massie GL (2008) The Encyclopedia of ancient natural scientists. The Greek tradition and its many heirs. Routledge, London
[46] Dioscoride. I.77
[47] Celso.V. 6,
[48] Pelag.Veter. XXXI
[49] Galeno In Kühn C.G. (1821– 1833, ristampa 1964– 1965; 1986) Claudii Galeni Opera omnia , 20 vv. in 22 parts. Leipzig
[50] Teofrasto (Historia Plantarum)
[51] Teofrasto (Historia Plantarum)
[52] Teofrasto (Historia Plantarum)
[53] Rufus (Hipp. Affect. \\’a4 52, t. VI, p. 262), Galeno in Kühn C.G. Op. Cit.
[54] Galeno Antid . 2.17 [14.203 K.] in Kühn C.G. Op. Cit.
[55] Galeno CMLoc 8.5 [13.179– 180 K.] in Kühn C.G. Op. Cit.
[56] Galeno Antid. 2.10 [14.158– 159, 161– 162 K.] in Kühn C.G. Op. Cit.
[57] Galeno CMLoc 7.2 [13.28– 30 K.]) in Kühn C.G. Op. Cit.
[58] Galeno, CMLoc 7.2 [13.31–32 K.] e CMGen 5.12 [13.835 K.] in Kühn C.G. Op. Cit.
[59] Asklepiades Pharm., in Galeno CMGen 7.6 (13.973–974) in Kühn C.G. Op. Cit.
[60] Galeno, CMLoc 7.2 (13.71 K) in Kühn C.G. Op. Cit.
[61] Kühn C.G. Op. Cit. De Compositione Medicamentorum secundum Locos. 9.4 (13.278)
[62] Iris pallida subsp. illyrica (Tomm. ex Vis.) K.Richt
[63] Askeliades Pharm., in Galen Antid.2.12 (14.177 K.) in Kühn C.G. Op. Cit.
[64] Asklepiades Pharm., in Galen CMGen 7.6 (13.967 K.) in Kühn C.G. Op. Cit.
[65] 30 citazioni in Scribonius Largus XCIV in Sconocchia S. (1981) Per una nuova edizione di Scribonio Largo
[66] 5 citazioni in Galeno, De Simpl. VIII.XVIII.30 in Kühn C.G. Op. Cit.
[67] 4 citazioni in Marcellus, XV. 6
[68] 3 citazioni in Dioscoride, I. 77
[69] 2 citazioni in Marcellus, IX. 18.
[70] cfr. Celso.V.22. 7.1
[71] Celso V.20.5
[72] Celso .V.21.1.
[73] 4 citazioni in Scribonius Largus CXXXIVT in Sconocchia S. (1981) Op. Cit.
[74] Scribonius Largus CCLXIX In Sconocchia S. (1981) Op. Cit.
[75] Celso.V.24.1.
[76] Plinio H.N.XXVI.109
[77] De Simpl. VIII.XVIII.30
[78] Serenus Sammonicus I.11.
[79] Scribonius Largus CCLXVII In Sconocchia S. (1981) Op. Cit.
[80] Dioscoride. I.77.
[81] Scribonius Largus. CLXXVII in Sconocchia S. (1981) Op. Cit.
Otto seminari otto

Negli anni ho tenuto vari corsi sulle piante medicinali, primariamente indirizzati a studenti/esse di Tecniche Erboristiche, ad erboristi/e, a farmacisti/e e medici.
In fase di progettazione dei corsi ho sempre cercato di inserire una parte dedicata alla metodologia di ricerca e agli strumenti di analisi delle evidenze, ma questo approccio non ha mai incontrato un grande successo, e posso capirne il perché: a causa del tempo limitato che i professionisti riescono a dedicare all’aggiornamento, spesso la tentazione è di accumulare quante più informazioni possibili da poter spendere praticamente nel lavoro quotidiano. Discorsi teorici sulla validità delle evidenze, sul loro reperimento, sulla loro valutazione possono sembrare solo ostacoli e ritardi inutili, in fondo chi viene a seguire il corso implicitamente considera il docente come fonte attendibile.
Io penso invece che, in un’ottica che vada al di là dell’immediatamente utile, tale approccio vada ripensato. Proprio perché il tempo (ed i soldi) sono limitati è utile sviluppare in proprio gli strumenti che ci permettono di formarci da soli una opinione sulle informazioni che riceviamo, senza dovere ogni volta iscriversi ad un altro corso che darà informazioni sparse che inevitabilmente saranno obsolete nel giro di relativamente poco tempo. Se questo discorso vale per tutti i professionisti, vale a mio parere ancora di più per gli erboristi.
A differenza di medici e farmacisti, chi lavora con le piante medicinali ha un corpus di evidenza sul quale basare le proprie decisioni più limitato e di qualità più variegata. Inoltre le fonti di evidenza sono più diversificate, non essendo limitate a dati sperimentali e clinici, ma comprendendo anche dati storici ed etnobotanici. Gli erboristi non hanno quindi a disposizione facili ed esaustivi formulari, e devono spesso valutare da soli l’importanza di un dato, e devono inoltre possedere diverse competenze per decifrare lo scenario.
Inoltre l’impressione che mi sono fatto in questi anni è che spesso chi lavora nel campo erboristico mantiene un atteggiamento diffidente e pregiudiziale nei confronti della “Scienza”.
Seppure possa capire da dove proviene questo sentimento, credo che esso sia ingiustificato, e che in realtà impedisca di mettere in campo critiche serie al modo in cui la ricerca viene fatta. Come non mi stanco di ripetere, l’unico modo per pretendere che i dati storici sulle piante medicinali vengano presi seriamente in considerazione è di essere scientificamente stringenti e metodologicamente esigenti (ho coperto questi argomenti in una serie di post su questo blog, in particolare in Indici quantitativi, Indicazioni tradizionali, e Uomo e piante)
Tutto questo per dire che sono molto contento che la S.I.S.T.E. abbia accettato la mia proposta di un corso di otto seminari sulle piante medicinali, i cui due primi appuntamenti saranno interamente dedicati alla problematica dei metodi di ricerca scientifica, e al problema di come valutare ed utilizzare i dati provenienti da storia della medicina ed etnobotanica.
I seminari si terranno a Milano, presso la sede della S.I.S.T.E., i lunedì, dalle 10.00 alle 13.00 e dalle 14.00 alle 17.30, con il seguente calendario: 15 Aprile; 13 Maggio; 27 Maggio; 10 Giugno; 16 Settembre; 14 Ottobre; 11 Novembre; 16 Dicembre.
E’ possibile scaricare il programma dei seminari e la domanda di iscrizione qui.

Il corso sarà diviso in due parti, la prima dedicata, come già accennato, alle basi della ricerca, mentre la seconda cercherà di delineare lo stato dell’arte sulle piante medicinali che hanno una base di evidenza più solida, dividendo gli argomenti per apparato.
Di seguito il programma completo.
Seminario 1. (15/4) La ricerca in fitoterapia.
Le basi: la logica della ricerca.
Scienza: non una vacca sacra e neppure un “discorso” tra tanti. Demistificare per valutare.
Breve introduzione alla scienza con il metodo del riepilogo storico.
Cosa è il metodo scientifico? Ovvero, esiste un metodo scientifico? Alcune ragioni per dubitare ma non per disperare. Tentativi di inquadramento dei termini chiave.
Il problema della demarcazione, ovvero, di chi mi devo fidare anche se fa male?
Le basi: la logica della medicina
– Cause
– Malattia e normalità
– Credere, dubitare e sospendere il giudizio
– Prove
– Bias
– Confounding
Seminario 2. (13/5) Gli strumenti a nostra disposizione
Le fonti di informazione a nostra disposizione e più rilevanti per la fitoterapia
– Ricerca storica ed etnobotanica
– Fitochimica ed evoluzione
– Studi in vitro ed in vivo
– Studi clinici
– Metastudi
– Limiti e punti di forza dei vari studi.
L’interpretazione dei dati
– Cenni di epidemiologia
– Come leggere gli studi e come attribuire valori di evidenza e di rilevanza agli studi
– Come costruire una gerarchia delle evidenze
– Cenni ai problemi più generali della ricerca.
Seminario 3. (27/5) Stato dell’arte della ricerca sulle piante.
– Una visione sullo stato dell’arte: definizioni.
– Le piante con maggiori livelli di evidenza per l’efficacia
– I dati tossicologici
– Interazioni negative e positive
Gli utilizzi delle piante e gli apparati.
Ogni seminario presenterà brevi cenni di fisiopatologia dell’apparato/sistema in questione, ed esaminerà le piante rilevanti che abbiano un sufficiente supporto clinico e sperimentale, oltre a suggerire quali altre piante potrebbero essere utili seppure con un supporto minore.
Seminario 4. (10/6)
– Tonici ed adattogeni
– Antibiotici, immunomodulanti.
Seminario 5. (16/9)
– Apparato gastrointestinale: problemi funzionali (dispepsia, sindrome dell’intestino irritabile, reflusso), gastrite, stipsi, diarrea, disbiosi, problemi epatobiliari
– Apparato genito-urinario: le infezioni del tratto urinario, disturbi funzionali della minzione, iperplasia prostatica benigna, calcolosi
Seminario 6. (14/10)
– Apparato cardiocircolatorio: ipertensione, aritmie, palpitazioni, insufficienza venosa cronica.
– Metabolismo: dislipidemie, disglicemie, prediabete, sindrome metabolica
Seminario 7. (11/11)
– Apparato muscoloscheletrico: dolori reumatici, traumi, dolori muscolari
– Apparato nervoso periferico e centrale: ansia, stati depressivi, insonnia,
Seminario 8. (16/12)
– Apparato tegumentario: acne, eczema, psoriasi, micosi cutanee.
– Apparato respiratorio: le malattie da raffreddamento, le bronchiti, la tosse, otite, sinusite, rinite allergica
Il mattone 2.0. La seconda edizione del manuale sugli olii essenziali è uscita.

Dieci domande di scienza ai politici, e poche risposte
Il gruppo Dibattito Scienza è nato su Facebook grazie all’iniziativa di ricercatori, giornalisti, docenti, giornalisti e blogger scientifici impegnati a portare avanti un dibattito pubblico sul ruolo della scienza nella politica italiana. Il gruppo ha pensato che il modo migliore per capire quali fossero gli impegni dei gruppi politici rispetto alle problematiche scientifiche fosse quello di porre ai responsabili delle domande specifiche, in modo da poter valutare le loro risposte. Dieci domande sono state selezionate, in maniera democratica, tra le molte proposte nate all’interno del gruppo di Facebook, che conta ora 1400 iscritti.

Esiste anche un omonimo sito web, dove è possibile leggere le dieci domande, illustrate in un video creato da un membro del gruppo, intitolato Le dieci domande di Dibattito Scienza. Esiste anche un video che illustra le dieci domande (e nel futuro le risposte date dai politici, vedi sotto) nel linguaggio dei segni italiano (PoLIS), creato da Claudio Ferrara, per contribuire ad includere le persone sorde nel dibattito.

Le dieci domande sono state inviate ai vari gruppi politici e ad i loro responsabili, ai quali è stato dato tempo sufficiente per offrire delle risposte ragionate. Purtroppo, come scrive Marco Cattaneo in questo articolo, solo tre leader hanno risposto, Bersani, Giannino e Ingroia, mentre Monti, Berlusconi e Grillo non lo hanno fatto, portando a loro discolpa varie scuse (a voi giudicare se siano credibili). Certo è scorante che il 50% dei leader abbia scelto di snobbare domande a mio parere importanti e molto rilevanti (qui un commento molto critico in lingua inglese di Giovanni Perini, e qui una pagina dove lo stesso autore pone i presupposti metodologici per l’esame delle risposte date dai leader).

Aspettiamo di leggere le risposte, possiamo ancora partecipare esigendo chiarimenti da chi non ha risposto…

Indici quantitativi in etnobotanica
Nel post precedente (qui) ho iniziato a parlare del problema della valutazione e dell’utilizzo dei dati etnobotanici e storici. Ho analizzato uno dei punti critici del processo di indagine, cioè la valutazione quantitativa della segregazione delle piante medicinali nelle famiglie botaniche, concludendo che questa segregazione esiste e sembra indicare una scelta non casuale delle piante da parte dei gruppi umani. Quali poi siano le ragioni per questa scelta è naturalmente un problema più complesso, e che quasi certamente non permette risposte mono-causali.
E’ stato proposto [1] che gli schemi di classificazione che osserviamo nelle e tra le società siano il risultato di:
- predisposizioni cognitive universali risultanti dall’evoluzione.
- l’oggettiva struttura tassonomica del bioma locale che non possiamo fare a meno di riconoscere.
- interpretazioni culturali relative.
- meri artefatti dei metodi di ricerca.
Il sapere tradizionale
Ma prima di affrontare questo argomento è necessario evocare il convitato di pietra di questa discussione, cioè il “sapere tradizionale” (o sapere ecologico tradizionale, o sapere locale, come è stato variamente definito). Fino ad ora, e nel post precedente, per comodità di trattazione ho usato questo termine (d’ora in poi ST) come se non esistessero ambiguità rispetto alla sua definizione, alla sua estensione, alle sue origini. Ma è utile soffermarci di più sulla sua articolazione all’interno della ricerca in etnobotanica, perché è essenziale per l’esplorazione del rapporto tra dati storico-etnobotanici ed efficacia biologica, ed inoltre perché è proprio sull’interpretazione del termine e sul sull’utilizzo da fare del “sapere tradizionale” che spesso casca l’asino della discussione erboristica/fitoterapica.
Partiamo intanto con una definizione preliminare tratta da un articolo di Victoria Reyes-García del 2010. L’autrice definisce il ST o i sistemi di sapere tradizionale come: “il sapere sulle risorse e le dinamiche dell’ecosistema, e le pratiche di gestione ad esso associate esistenti tra i membri della comunità che, giornalmente e per lunghi periodi di tempo, interagiscono per il proprio benessere e per la coesistenza con l’ecosistema stesso”. Secondo l’autrice il ST include non solo informazioni sugli usi umani di piante ed animali, ma anche sistemi di classificazione, osservazioni sull’ambiente locale e un sistema di utilizzo e gestione delle risorse, oltre a credenze su esseri non umani, sovrannaturali, e sulle relazioni che essi intrattengono con la società. In definitiva il sapere tradizionale deve essere inteso come in modo di comprendere il mondo o la “cultura”.Esso rappresenterebbe un tratto culturale adattivo per le popolazioni che favorisce la loro sopravvivenza, la produzione di cibo, la costruzione di ripari e in genere il controllo sulle proprie vite. Verrebbe sviluppato e continuamente adattato ad un ambiente in continuo cambiamento, e verrebbe passato di generazione in generazione non isolato bensì strettamente intrecciato a valori culturali ed etici.
L’altro
Vista questa definizione, torniamo a bomba al problema dello status dei dati storici ed etnobotanici. Quello che a mio parere è uno dei problemi più diffusi in questo ambito è la tendenza a polarizzare i termini del dibattito seguendo una antica tendenza della discussione sull’altro o sull’alterità, cristallizzata dall’antropologia settecentesca intorno all’alternativa “buon selvaggio” (preservato dalla corruzione della civiltà grazie alle sue doti naturali) o “cattivo selvaggio” (immerso nella miseria e depravazione a causa della sua ignoranza e pigrizia).
Succede infatti spesso che l’altro erboristico (sia esso il medico antico che seguiva i dettami della sua tradizione di medicina colta, o sia esso il guaritore contemporaneo che in una società distante utilizza rimedi della foresta) venga costruito secondo una immagine idilliaca, con un discorso impressionistico e poco rigoroso. Si richiama, con modalità talvolta ingenua e nostalgica, un passato nel quale si potrebbero ritrovare le origini più vere, la vicinanza alla fonte, qualcosa di “originario” che il presente, il progresso e la modernità ci hanno tolto. Oppure si cerca nelle popolazioni esotiche e nelle loro culture “la silhouette mobile e vaga di un selvaggio che, più vicino di noi alla natura, avrebbe rifiutato in anticipo tutto ciò che ci opprime e del quale si troverebbe ancora traccia, ricordo o testimonianza nella foresta amazzonica o nel deserto australiano” (vedi ad esempio Marc Augè).
Termini che vengono spesso usati in questo contesto sono tradizione, radici, origine, memoria, ecc., ma raramente gli autori che li usano si fermano a pensare al perché essi vengano usati, ed in che modo. Questo ragionamento schematico e dicotomico, etnocentrico al rovescio, contribuisce ad imprigionare l’altro, a sottometterlo alla nostra rappresentazione. Spesso in questo dibattito si fa uso del termine e della metafora delle radici [2], che richiama il tema delle origini, che in quanto origini sembrano più importanti, imprescindibili, contenenti in nuce ciò che da esse si svolge [3]. Ma come dice Galimberti:
“Essere più vicini alla fonte non significa custodire qualcosa di “originario”, ma essere semplicemente all’inizio di un processo: la storia, che si compie facendosi, e non abolendola dissetandosi alla fonte. All’inizio c’è solo l’avvio, e non il senso nascosto, o il silenzio custodito da ciò che in seguito si dispiegherà. E solo il rifiuto del mondo che viviamo può far ritenere che il mondo antico, con il suo corredo di simboli, disponga di segni più veri. Ma rifiuto e nostalgia sono i moti dell’anima di chi disabita il mondo che per sorte si trova ad abitare, non sono certo criteri di giudizio, ne tantomeno sentieri di verità”.
Quantificazione
Fatta questa doverosa premessa circa l’atteggiamento metodologico da tenere quando siamo confrontati da dati storici ed etnobotanici, rimane l’aspetto tecnico, interno diciamo all’etnobotanica. Cosa significa il termine sapere tradizionale o i suoi cognati? E’ possibile quantificarlo? E se si, come?
La quantificazione del sapere tradizionale è stata tentata attraverso l’utilizzo di indici di misura dell’importanza culturale delle piante, i cosiddetti indici di Importanza Culturale Relativa [RCI]. Questi indici quantitativi si usano in etnobotanica per comparare usi e importanza culturale dei differenti taxa. Sono stati usati in vari studi e la loro utilità risiede in prima istanza nel fatto che su di essi si possono effettuare analisi statistiche di vario tipo per comparare diverse specie tra loro, zone vegetazionali, habitus, taxa, ecc. Essi inoltre permettono di ottenere valori numerici integrabili ad altri indici (tassonomici, fitochimici, ecc.) utilizzabili per comparazione trans-culturali e per testare differenti ipotesi.
Gli indici RCI si sono moltiplicati negli ultimi anni, ma mi soffermo in questo momento su tre gruppi di indici che sono particolarmente importanti.
1. Indici di totalizzazione degli usi
Semplici indici enumerativi, che elencano usi e non usi per ogni pianta. Un esempio è UT

Dove UT è pari alla semplice sommatoria di tutti gli usi conosciuti per ogni specie, che possono essere categorizzati per utilità, per taxon vegetale o per tipo vegetazionale. Questi metodi non tentano di misurare i livelli di importanza per i differenti usi e non tengono conto del consenso tra gli informatori. Il taxon più importante è semplicemente quello con le maggiori citazioni d’uso. Dal punto di vista della possibilità di catturare la complessità dell’oggetto sapere tradizionale (e della misura dell’importanza culturale) questi indici non offrono molto, e dal punto di vista della rilevanza statistica e della possibilità di testare delle ipotesi sono i meno efficaci. Non registrando la provenienza dell’informazione (da quale informatore) non permettono di valutare la variabilità intraculturale. Non tenendo in conto l’esistenza di livelli diversi di importanza, il metodo è eccessivamente sensibile all’intensità della campionatura (una pianta con molti utilizzi tutti poco importanti nel gruppo studiato peserebbe di più di una pianta con meno utilizzi ma molto più importanti). Per ovviare almeno in parte a questi deficit, sono stati sviluppati dei metodi più sofisticati, come quelli detti di assegnazione soggettiva dell’importanza.
2. Indici di assegnazione soggettiva
Indici simili a quelli precedenti, ma con modificatori di importanza basati sulle valutazioni e sulla conoscenza del contesto da parte del ricercatore. Questi indici pesati permettono la misura dei gradi di importanza ma introducono un pregiudizio del ricercatore che rende più difficile l’utilizzo degli indici, ad esempio nella analisi bibliografica. Un esempio è quello del Valore d’Uso (UVs)
UVs deriva da UT ma somma i punteggi generati dal ricercatore per ogni utilizzo (importante = 1 punto; poco importante = 0,5 punti).
Gli indici che sono stati più influenti nei decenni recenti sono però senza dubbio stati gli indici di consenso.
3. Indici di consenso tra gli informatori
Indici basati sul consenso tra gli informatori, con pesi dati agli usi generati dal ricercatore o dall’informatore. Questi indici si basano sulla teoria del consenso culturale (CCT), una teoria antropologica sviluppata per stimare la risposta culturalmente corretta in differenti domini del sapere tradizionale. La CCT parte dagli assunti che esista una risposta culturalmente corretta per ogni domanda [4], che il sapere consista nell’accordo tra informatori [5], e che la probabilità che un informatore risponda in maniera corretta ad una determinata domanda sia il risultato della sua competenza in quel dominio di sapere [6]. Si tratta quindi di un metodo che misura il sapere in termini di congruenza con un modello esplicativo proprio del gruppo studiato. Da ciò deriva l’ipotesi che maggiore la salienza di una pianta o di un suo utilizzo in una comunità, maggiore sarà la frequenza di citazione della pianta.
Qui sotto riporto alcune delle formule più usate.
1. Valore d’uso delle specie per un informatore:
Dove UVis = numero di usi menzionati per la specie s dall’informatore i; n is = numero di interviste nelle quali l’informatore i menziona un uso per la specie s.
2. Valore d’uso di una specie per tutti gli informatori

Dove ni = numero totale di informatori intervistati per la specie s. Questo indice misura il numero di usi attribuiti ad un taxon relativo al numero di informatori che citano il taxon, cioè misura l’importanza del taxon se per importanza intendiamo la sintesi degli usi. Alcuni autori hanno infatti riscontrato una correlazione positiva tra numero di informatori che considerano importante una specie s, l’indice UV, e il numero di utilizzi, ed hanno concluso che l’importanza è una sintesi della molteplicità degli usi di un taxon. Altri autori preferiscono legare l’importanza sia al numero di usi sia a quanto bene è conosciuta la pianta.
UVs può essere ritenuta rilevante quando tanti informatori citano molti utilizzi, ma può essere fuorviante se vi è un solo informatore che cita molti utilizzi, oppure se una pianta è oggettivamente molto importante, ad esempio una pianta simbolo stesso della società studiata, ma ha pochi usi. Teoricamente gli indici basati sul consenso degli informatori dovrebbero favorire quei taxon con un elevato livello di consenso in una cultura, ma un indice come UV è ancora molto crudo.
3. Metodo del punteggio dell’informatore
All’uso di una pianta viene assegnato dall’informatore un punteggio variabile da 0,5 (utilizzabile ma sub-ottimale) a 1,5 (quasi ottimale) in cinque categorie. Questi punteggi vengono sommati per ottenere un punteggio finale, per una singola intervista, nella forchetta 0-7,5. ISis si calcola come il punteggio medio per tutte le interviste, e ISs si ottiene come la media tra i valori d’uso per tutti gli informatori.
Criticità
Tutte queste tecniche condividono l’assunto che gli indici misurino il sapere tradizionale, e che l’estensione del sapere tradizionale su una pianta in una data cultura ci dia una misura indiretta dell’importanza culturale percepita di tale pianta in maniera più oggettiva degli altri indici. Inoltre, quando gli indici vengono utilizzati a scopo euristico, per delimitare taxa specifici per la ricerca etnofarmacologica, ci si basa sull’assunto che vi sia un legame tra importanza culturale, sapere tradizionale, efficacia percepita e potenziale farmacologico.
Ognuno di questi passaggi presenta delle criticità.
- Il rapporto tra indici RCI ed efficacia percepita potrebbe non essere lineare. Vi è ad esempio il ruolo della disponibilità delle piante che può confondere questo rapporto.
- Esistono molte discrepanze tra dati ottenuti con metodi differenti, discrepanze che rivelano come il sapere tradizionale comprenda molte dimensioni e campi differenti, rendendo difficile incapsularlo in un’unica definizione derivante da un unico metodo.
- Esistono discrepanze tra “sapere attivo” (quali piante vengono usate dalle persone) e “sapere passivo” (cosa le persone sanno sull’utilizzo delle piante)
- La correlazione tra sapere e consenso potrebbe non essere lineare e semplice, e potrebbe dipendere:
4.1. dal fatto che stiamo studiando piante medicinali o piante alimentari o piante medicinali e alimentari.
4.2. Da chi decidiamo di intervistare come informatore (guaritore, bambini, uomini, donne, ecc.). Gli etnofarmacologi si sono quasi sempre concentrati sui guaritori professionisti perché li ritenevano i più profondi conoscitori della materia, ma se professionisti e gente comune non condividono lo stesso corpus di sapere, allora restringere la ricerca ad un solo gruppo limita e rende pregiudiziale il tipo di informazione raccolta
4.3. Dalla differenza tra sapere condiviso e sapere idiosincratico
Casagrande mette anche in dubbio l’assunto che le piante usate più di frequente siano anche quelle percepite come più efficaci. L’autore arriva a questa conclusione dopo avere riscontrato nel suo studio sul campo che:
- L’abbondanza di una specie è collegata alla frequenza d’uso, mentre la frequenza d’uso non è collegata all’efficacia percepita; secondo l’autore questo indica che le prime piante ad essere utilizzate in caso di malattia sono le più disponibili, le più abbondanti nella vicinità delle zone abitate, a prescindere dalla loro efficacia. Le piante più efficaci (efficacia emica) vengono usate solo in caso le prime non risolvano il problema. Visto che la severità dei sintomi può scemare anche senza intervento, è probabile che in molti casi le piante più efficaci non verranno utilizzate.
- L’efficacia percepita e, in misura minore, la frequenza d’uso, sono correlati alla distribuzione del sapere, ma l’organizzazione sociale, i fattori cognitivi individuali e distribuiti, i processi di trasmissione culturale strutturata e random danno forma al processo di disseminazione. A parte poche piante e malattie molto comuni, la distribuzione del sapere sarà spesso random o non prevedibile.
Questi risultati mettono in crisi il postulato di molta ricerca quantitativa che suppone che frequenza d’uso, distribuzione del sapere e/o consenso tra informatori si correli bene con l’efficacia percepita, e mette quindi in dubbio la correlazione tra indici RCI ed efficacia emica. I risultati metterebbero anche in dubbio l’ipotesi che le piante più disponibili siano più utilizzate perché conterrebbero più composti interessanti (come voleva Moerman): le piante più disponibili verrebbero più usate semplicemente perché sono più disponibili.
Sarebbe quindi meglio misurare direttamente l’efficacia percepita, ma anche il legane tra efficacia percepita e potenziale farmacologico non è netta, perché le informazioni variano tra le popolazioni, è quindi necessario comparare diverse comunità in aree geografiche diverse e preferibilmente lontane.
Quindi, secondo Casagrande i rapporti tra frequenza d’uso e abbondanza di una pianta non sono indicatori forti dell’efficacia percepita, mentre il consenso lo è, e comunque l’efficacia percepita ha un legame debole con il poitenziale famacologico se non viene analizzata a livello transculturale (vedi il prossimo post).
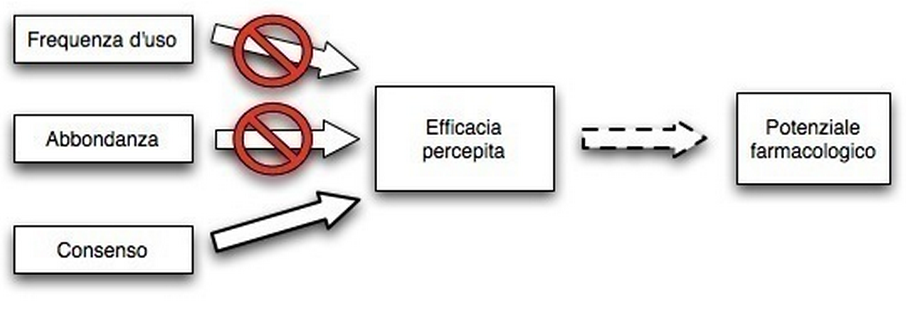
Questo non significa che, secondo Casagrande, le piante usate dalle popolazioni non siano mai efficaci, ma che gli schemi di distribuzione del sapere non rappresentano una corrispondenza ottimale tra bisogni indotti dalla malattia e i composti fitochimici disponibili nell’ambiente.
Il prossimo post si concentrerà su due articoli che descrivono due applicazioni molto diverse tra loro degli indici, ma che ci possono servire per capirne meglio l’utilità.
————————————————————————————————————————————————————————————————–
Note
[1] Casagrande, David 2004 Ethnobiology lives! Theory, Collaboration, and Possibilities for the Study of Folk Biologies. Reviews in Anthropology, vol. 33, pp. 351 to 370
[2] Una metafora molto potente perché mentre nessuno ha mai visto una tradizione o una identità, tutti hanno visto delle radici.
[3] Lo stesso concetto di tradizione viene presentato come monolitico e fisso. In effetti se non fosse presentato in questo modo non potrebbe svolgere il compito che gli viene richiesto, quello di “ancorare” le pratiche presenti ad un passato “naturale” che le giustifichi. Ma questa visione, di nuovo piuttosto ingenua, non rende conto del carattere costruttivo e dinamico della tradizione e della memoria collettiva che hanno bisogno di una serie di cornici di riferimento a carattere sociale che ne condizionano fortemente i contenuti. Al mutare dei quadri sociali muta la memoria. La memoria collettiva e la tradizione culturale si creano attraverso un processo di ricostruzione artificiale (vedi il Palio di Siena, la topografia leggendaria dei Vangeli in Terra Santa, la costruzione delle differenze etniche tra Hutu e Tutsi) (Halbwachs (1987) La memoria collettiva, Unicopli, Milano). Proprio gli antichi sembravano ben avvertiti del carattere dinamico e non monolitico della tradizione, incapace da sola a fondare una identità: Cicerone (De legibus, 2, 16, 40) racconta che un’ambasciata ateniese si recò a Delfi per chiedere ad Apollo quali riti sacri mantenere e quali no. L’oracolo rispose: eos quae essent in more maiorum, cioè “quelli conformi al costume degli antenati”, ovvero “tenetevi alla vostra tradizione”. Ma gli ateniesi tornarono poco dopo per ottenere maggiori delucidazioni sul significato dell’indicazione: infatti il costume degli antenati era mutato molte volte, quale era la tradizione che dovevano ritenere quella valida? Al che Apollo rispose: “la migliore”, rivelando che la tradizione non è ne fissa ne monolitica, cambia e si costruisce, e alla fine la scelta si basa su criteri utilitaristici, non sull’antichità.
[4] Nel senso che la realtà culturale, definita come la risposta data dalla maggior parte delle persone, è la stessa per tutti gli informatori (o le fonti di informazione, in caso si lavori su testi.
[5] Il livello di accordo tra informatori riflette il loro accordo congiunto
[6] Se consideriamo la competenza come la percentuale di riposte corrette.